Figures
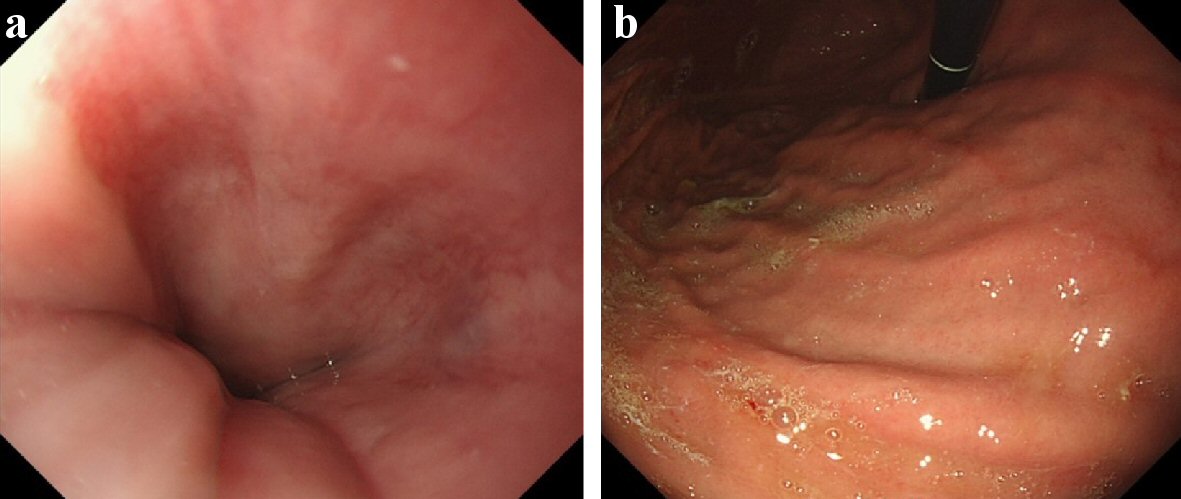
Figure 1. Esophagogastroduodenoscopy of December 2017, before radiotherapy. (a) Lower esophagus, 39 cm from the incisors. (b) Cardia of stomach. They were endoscopic findings of the area before performed radiotherapy for hepatocellular carcinoma (HCC). At this point, there were no inflammatory findings on the lower esophagus and the cardia of the stomach.
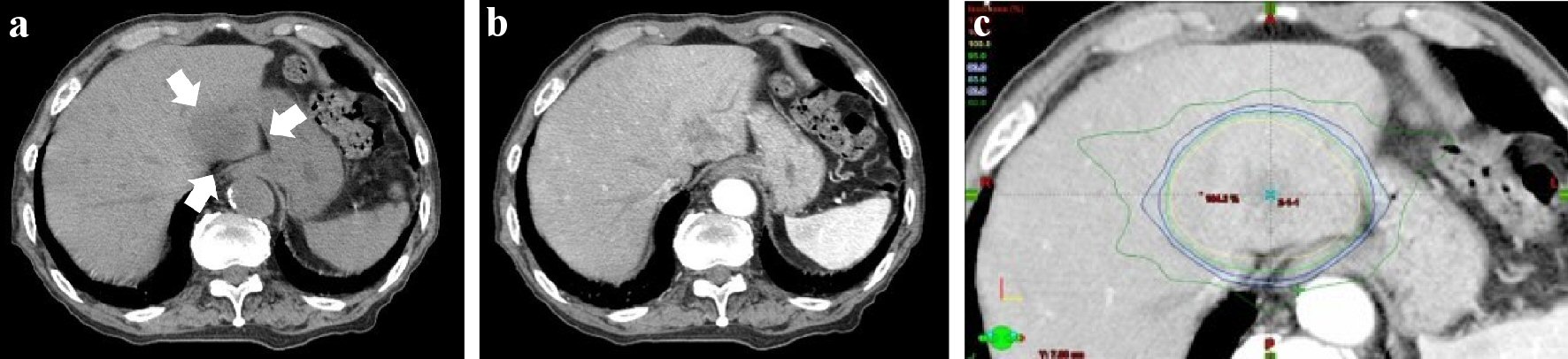
Figure 2. Abdominal computed tomography (CT) of December 2017, before radiotherapy. (a) Abdominal CT (plain). (b) Abdominal CT (contrast-enhanced; arterial phase). (c) Dose distribution (isodose distributions: yellow line 100%; inside/green line 95%; blue line 90%). There was a low density area (about 4 cm in size; white arrow) in hepatic segment 2 for abdominal plain CT. It was well-enhanced in the arterial phase for contrast-enhanced CT. The lesion was close to the gastroesophageal junction. The lower esophagus and the cardia of the stomach were included in the range of the radiation (yellow arrow head). The total dose to HCC was D0.5 cm3 = 49.0 Gy, the lower esophagus: D0.5cm3 = 48.4 Gy.
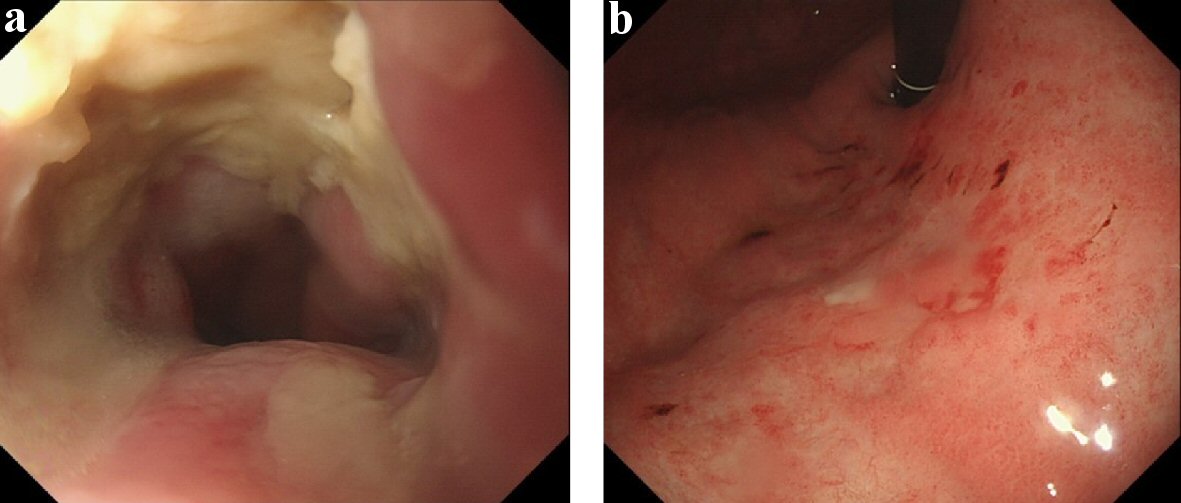
Figure 3. Esophagogastroduodenoscopy of June 2018, after radiotherapy. (a) Lower esophagus. (b) Cardia of stomach. There were semicircular esophageal ulcer with slight stenosis on the lower esophagus, 39 cm from the incisors, and localized gastritis with hematin on the cardia of the stomach.
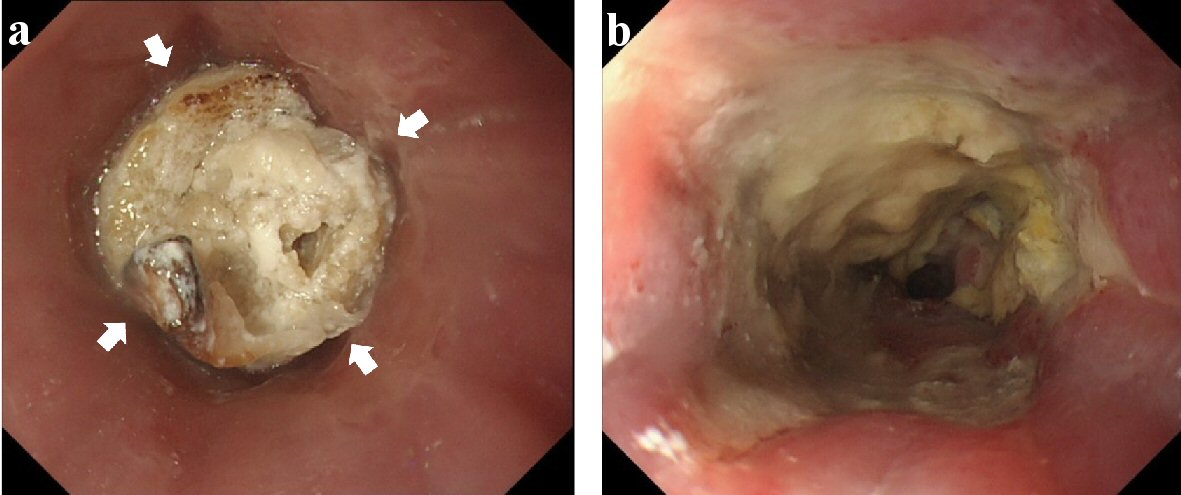
Figure 4. Esophagogastroduodenoscopy of July 2018, after radiotherapy. (a) Lower esophagus (before removal of foreign body). (b) Lower esophagus (after removal of it). Stagnated chicken was found in the lower esophagus (white arrow). After the removal, the range of the esophageal ulcer enlarged to the oral side.
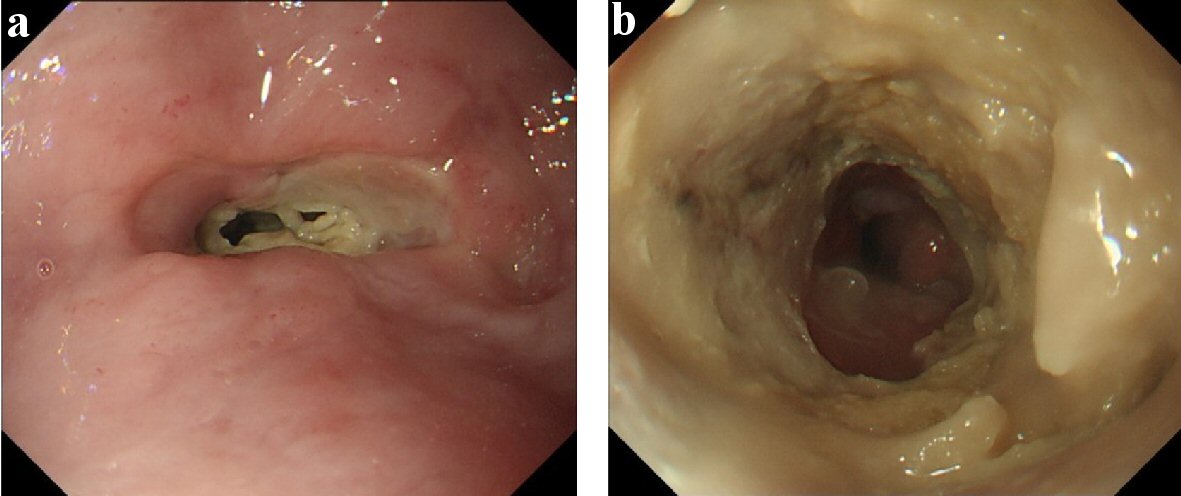
Figure 5. Esophagogastroduodenoscopy of August 2018. (a) Lower esophagus (before endoscope passed). (b) Lower esophagus (after it passed). Esophageal ulcer grew up for the circumferential lesion with the progression of stenosis. It was barely passed by GIF-H290 (8.9 mm (outer diameter); Olympus Medical Systems Corp., Japan).
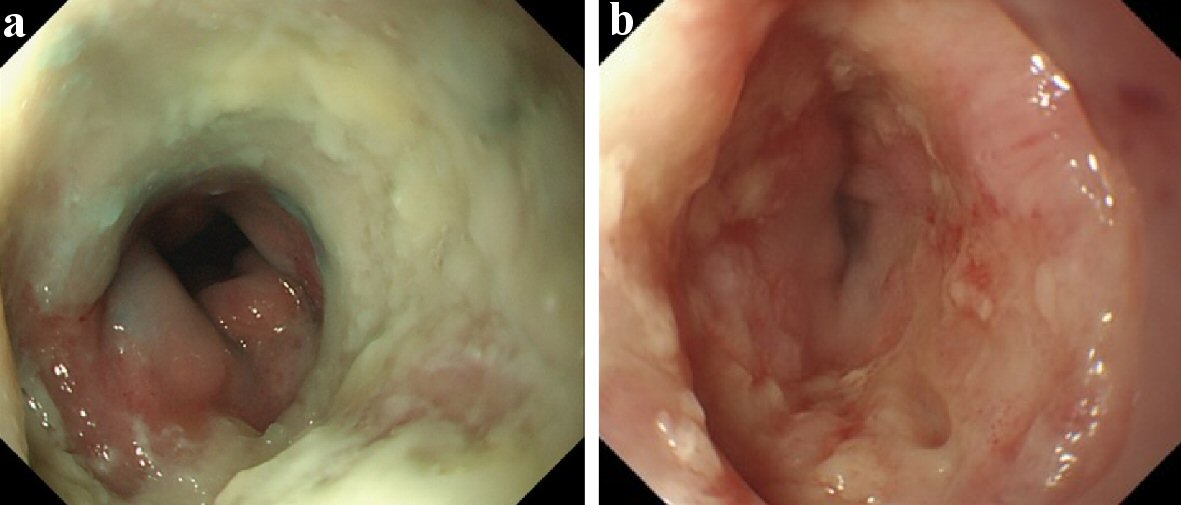
Figure 6. Esophagogastroduodenoscopy of September 2018 and March 2019. (a) Lower esophagus (September 2018). (b) Lower esophagus (March 2019). The esophageal ulcer was slowly improved by conservative therapy. It almost healed with moderate stenosis in March 2019.
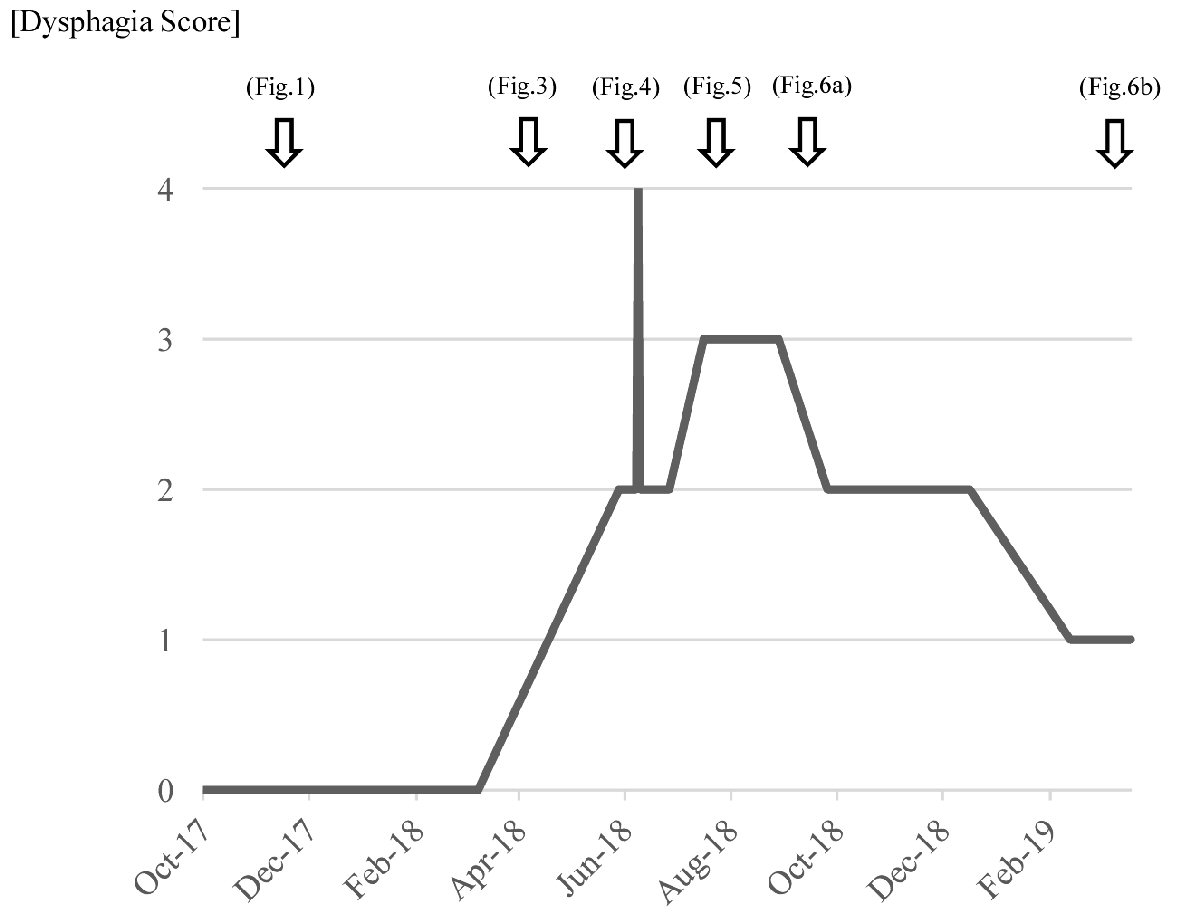
Figure 7. Changes in dysphagia score at different times. Dysphagia score: 4 = no passage (unable to swallow anything); 3 = very poor passage (able to swallow liquids only); 2 = poor passage (able to eat semi-solid foods); 1 = moderate passage (able to eat some solid foods); 0 = no dysphagia (able to eat normal diet).