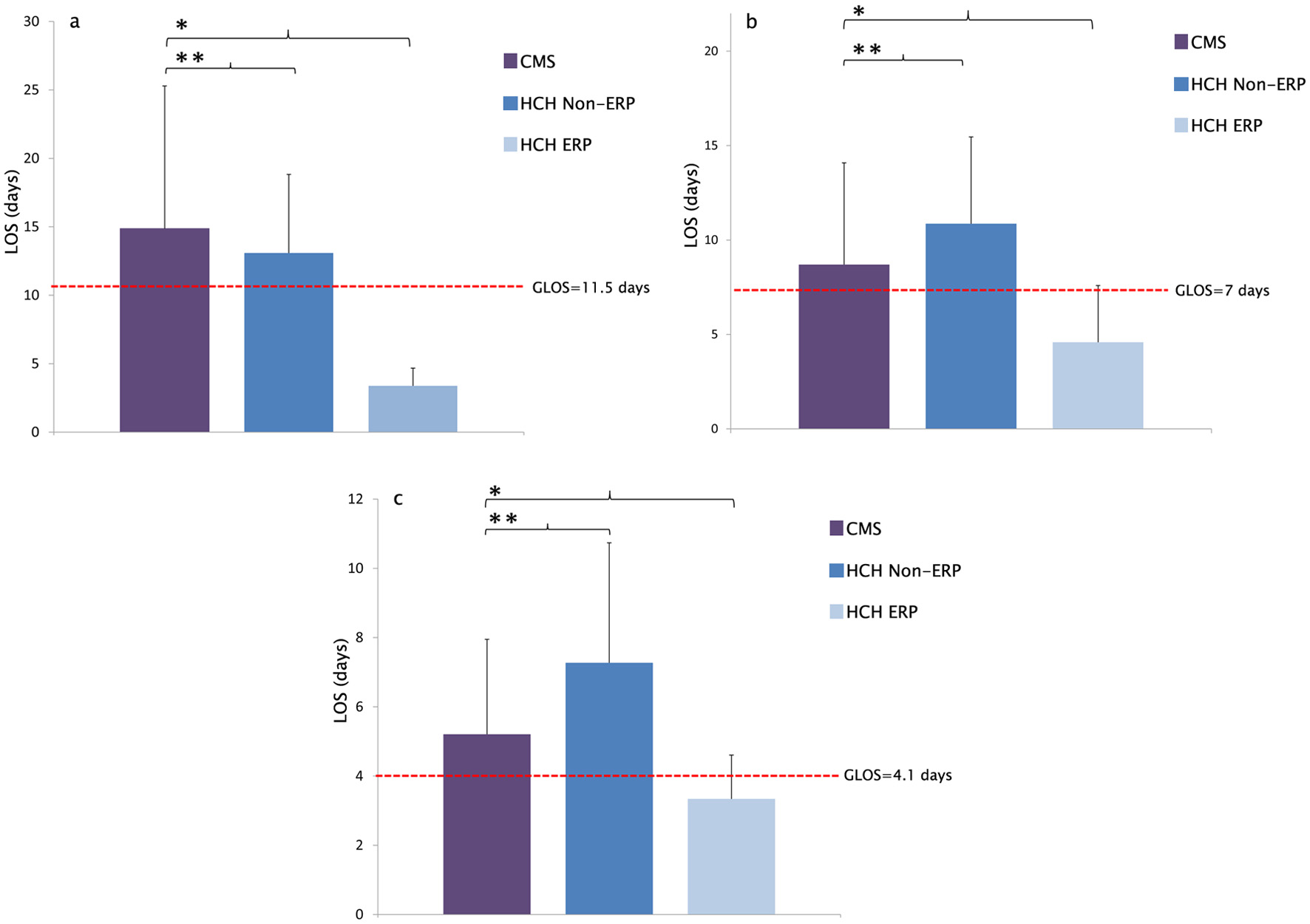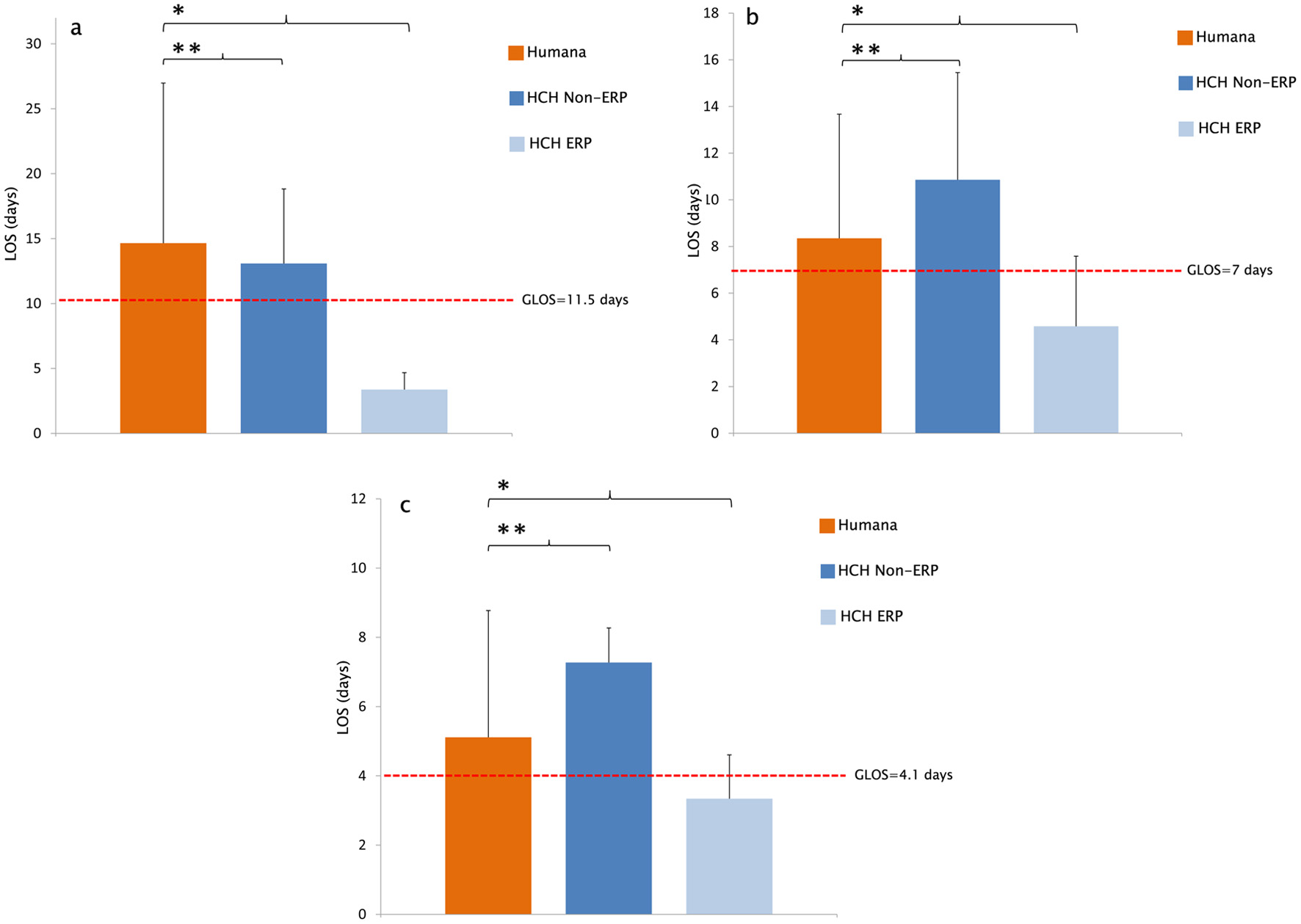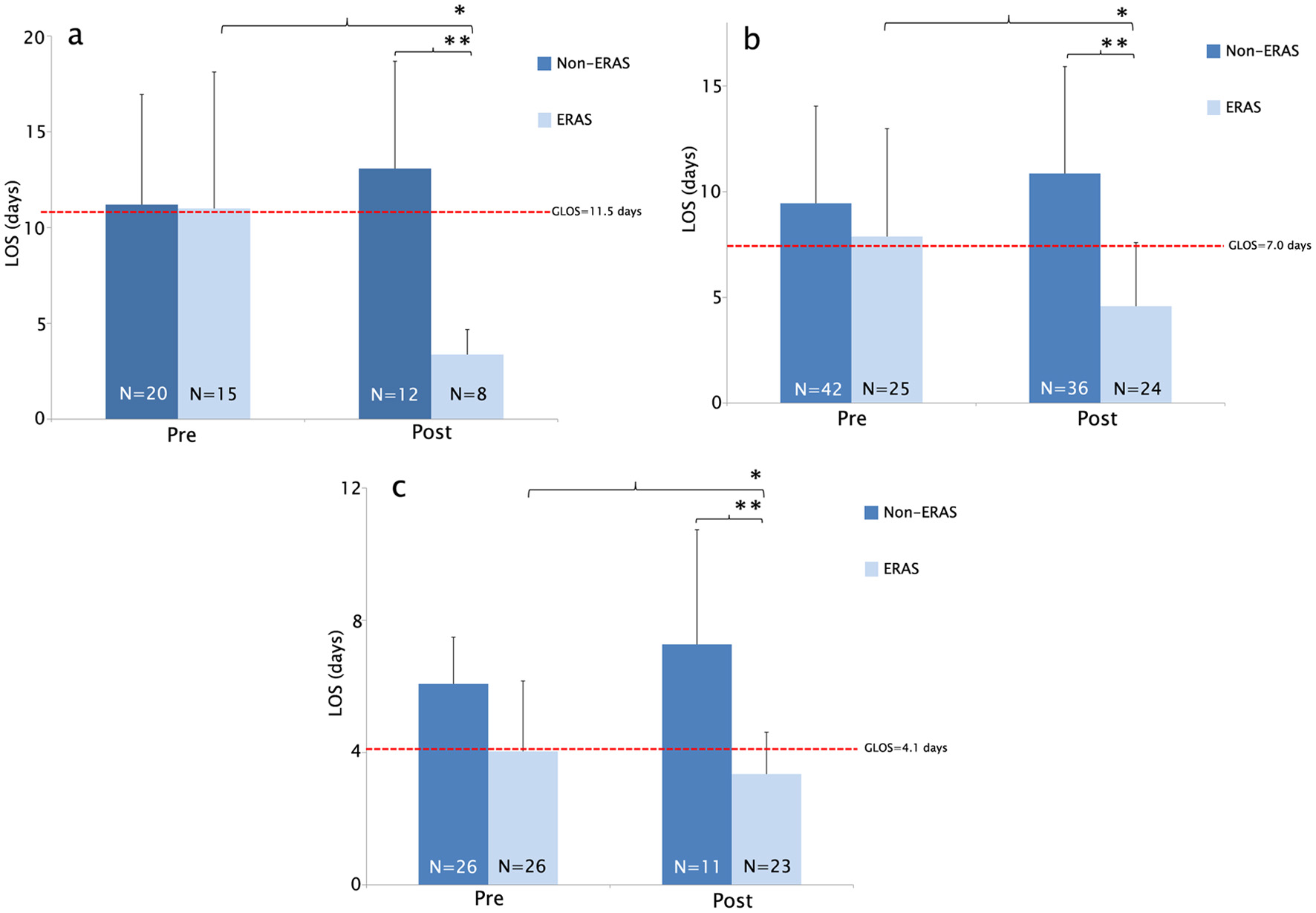
Figure 1. (a) Average LOS was significantly reduced in the ERP participating group DRG 329 at HCH. LOS significantly improved among ERP participating surgeons when compared before and after ERP implementation (*Reduction in LOS (days) 11.0 vs. 3.375, *P = 0.001). LOS significantly improved in patients undergoing ERP compared to patients undergoing non-ERP (**Reduction in LOS (days) 13.0833 vs. 3.375 (**P = 6.99 × 10-5)). (b) Average LOS was significantly reduced in the ERP participating group DRG 330 at HCH. LOS significantly improved among ERP participating surgeons when compared to before and after ERP implementation (*Reduction in LOS (days) 7.88 vs. 4.58 (*P = 0.008)). LOS significantly improved in patients undergoing ERP compared to patients undergoing non-ERP (**Reduction in LOS (days) 10.861 vs. 4.583 (**P = 1.31 × 10-7)). (c) Average LOS was significantly reduced in ERP participating group DRG 331 at HCH. LOS significantly improved among ERP participating surgeons when compared before and after ERP implementation (*Reduction in LOS (days) 4.03 vs. 3.34 (*P = 0.1689)). LOS significantly improved in patients undergoing ERP compared to patients undergoing non-ERP (**Reduction in LOS (days) 7.272 vs. 3.34 (**P = 0.004)). ERP: enhanced recovery protocol; DRG: diagnostic-related group; LOS: length of stay; HCH: Holy Cross Hospital.