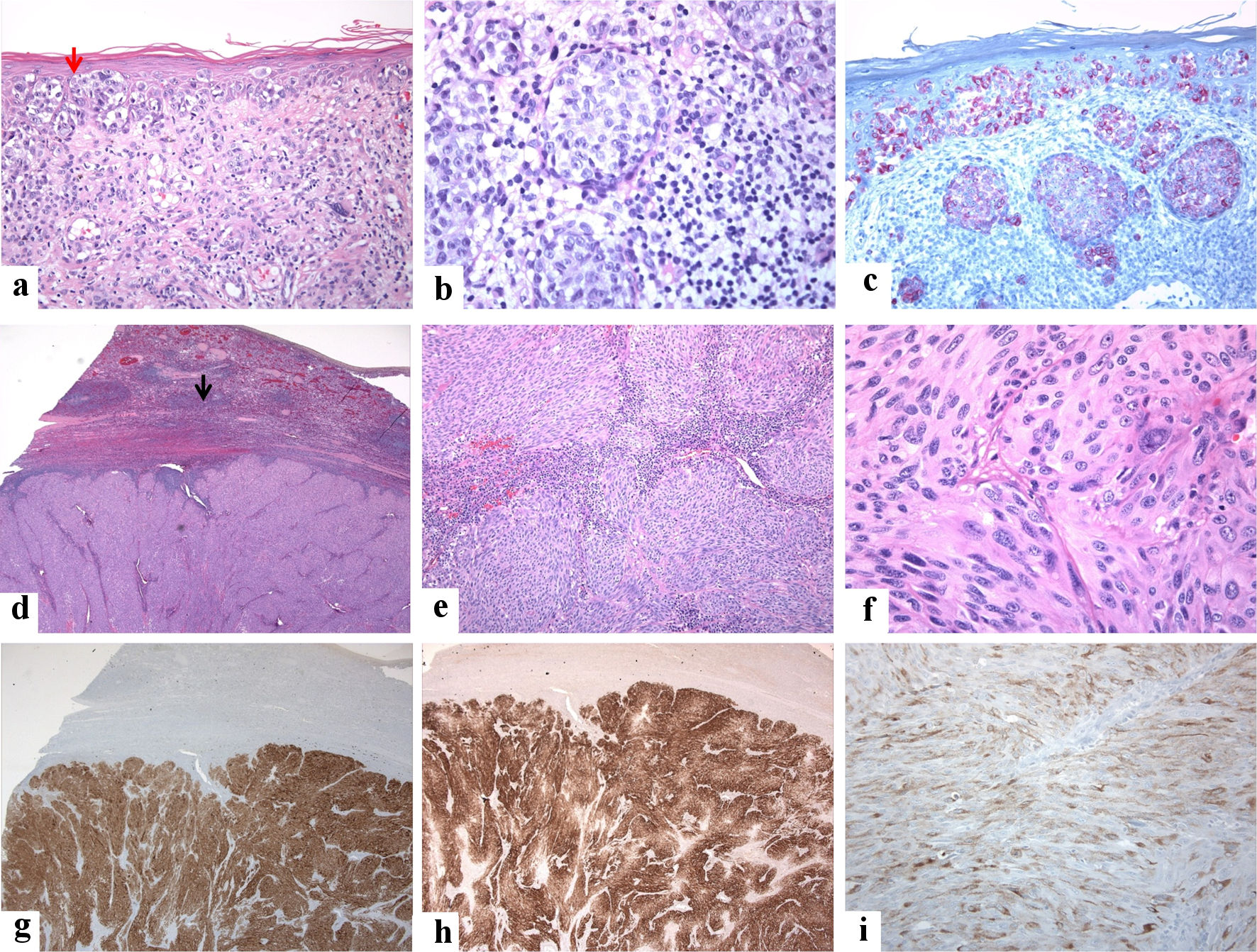
Figure 1. A 72-year-old male patient presented with vague mild pain in the left hypochondrium. He had a past medical history of malignant melanoma of the scalp that was treated with a wide local excision 25 years back (the tumor was grossly 1.0 cm in greatest dimension, microscopically Clark’s level IV, number of mitoses 1.0/mm2, without ulcerations or signs of regression, and all margins were negative). Clinical examination revealed no organomegaly or masses or skin lesions (apart from an old residual scar from the previous excision of melanoma on the scalp). Laboratory tests were unremarkable except for high lactate dehydrogenase (LDH) levels. Radiological investigations (ultrasound and magnetic resonance imaging (MRI)) revealed a solitary 4 × 3 × 3 cm solid lesion in the spleen suggestive of a neoplastic process. No other lesions are seen. A splenectomy was done, and postoperative recovery was uneventful. Grossly, the spleen weighed 185 g and measured 11 × 8 × 5 cm. Its cut section showed a well-defined subcapsular solid mass of 4 × 3 × 3 cm with a tan-white cut section and firm consistency. The masse was bulging into, but not breaching, the splenic capsule. The surrounding’s non-neoplastic splenic tissue was unremarkable. A single small lymph node (0.5 cm) with a pink cut section and soft consistency was identified in the helium. No evidence exists of BRAF-V600 (v-RAF murine sarcoma viral oncogene homolog B1) E/K mutation by amplification refractory mutation system (ARMS) analysis. The lymph node showed reactive changes. Investigations did not reveal any other site of metastasis. The patient has completed 1-year of follow-up without signs of residual or recurrent disease. The clinicopathological findings agree with the previous reports [13-16]. The immunohistological features of the patient are shown below. (a, b) From a cutaneous malignant melanoma of the scalp, malignant cells with pagetoid spread into the epidermis (red arrow) are shown. The tumor cells are arranged in a nesting pattern in the dermis. They have round nuclei and vacuolated and pink cytoplasm. Dermal host response in lymphocytic infiltrate is seen (hematoxylin and eosin-stained section, magnification (a) × 10, (b) × 20). (c): The tumor cells show patchy reactivity for human melanoma black-45 (HMB45) (magnification: × 20). (d, e) From the spleen, it is shown the replacement of the splenic parenchyma by malignant neoplasm and residual lymphoid cells at the periphery (black arrow) (hematoxylin and eosin-stained section, magnification: (d) × 4, (e) × 10). (f) The high-power view shows round, short spindly, and ovoid cells arranged in vague solid and fascicular patterns, the tumor cells with pink cytoplasm, and eosinophilic cytoplasm (hematoxylin and eosin-stained section, magnification: × 40). (g, h, i) The melanocytic markers highlight the tumor cells ((g): S100, (h): Melan A, and (i): HMB45) (magnifications: (g) × 4, (h) × 4, and (i) × 20). The tumor cells were positive for S100, Melan A, and HMB45. Negative stains included CD45 (leukocyte common antigen (LCA), CD10, CD30, P63, pancytokeratin (AE1/AE3), epithelial membrane antigen (EMA), cytokeratin 20 (CK20), cytokeratin7 (CK7), smooth muscle actin (SMA), synaptophysin, and desmin.