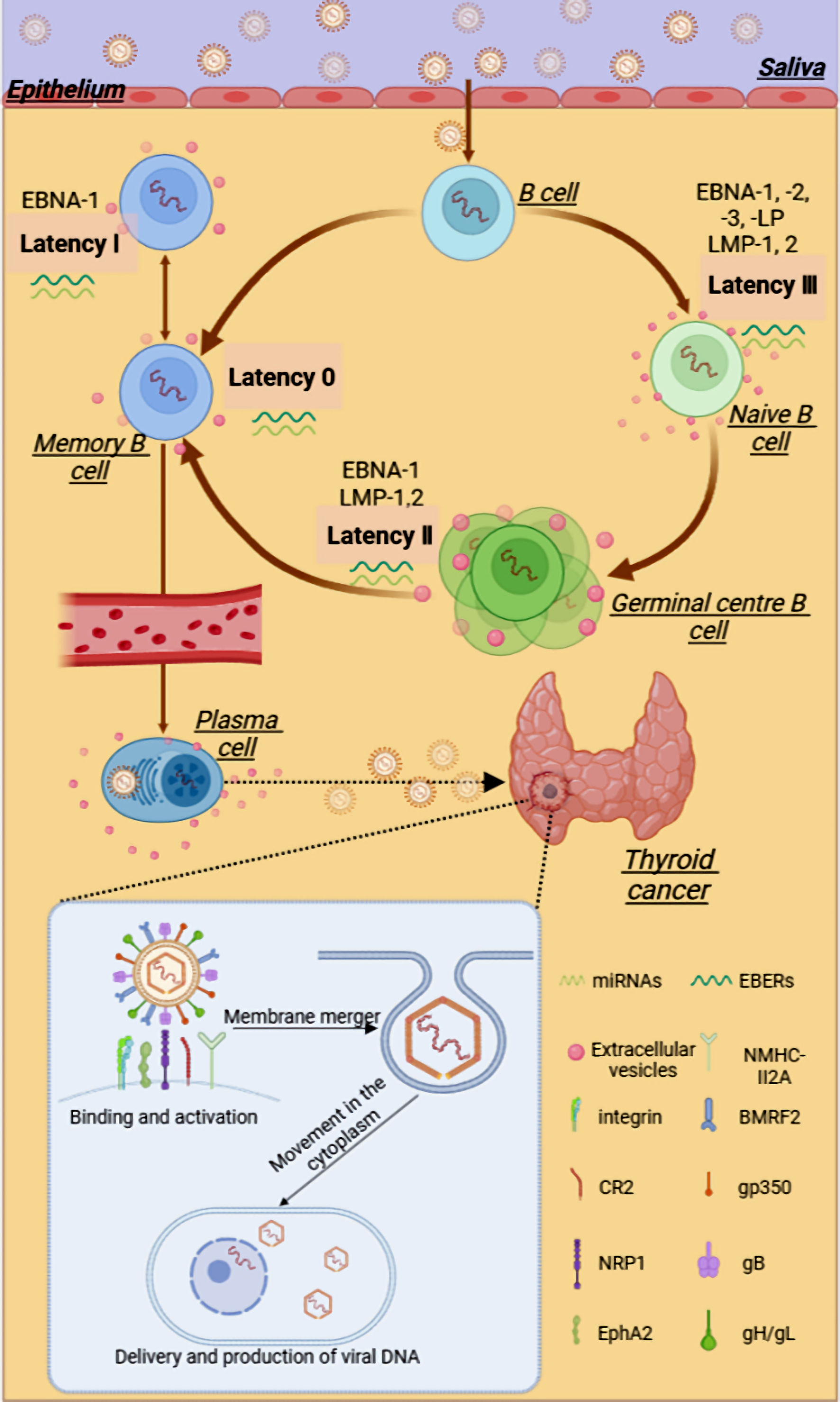
Figure 1. The possible relationship between EBV and thyroid cancer. EBV can be transmitted through saliva, passing through the oropharyngeal epithelium and tonsils, infecting lymphoid B cells, and subsequently infecting the initial B cells. After a complex series of latent infections, EBV may enter thyroid tissue through the blood circulation or lymphatic system. EBV can package various viral products, such as viral proteins and RNAs, into the extracellular vesicles to aid in the evasion of the host immune system and promote tumor progression within the TME. In the presence of multiple viral glycoproteins, EBV binds and activates receptors on cells, invading and proliferating within thyroid cells. gB: glycoprotein B; gH: glycoprotein H; gL: glycoprotein L; NRP1: neuropilin 1; EphA2: ephrin receptor A2; EBV: Epstein-Barr virus; EBNA1: Epstein-Barr virus nuclear antigen 1; EBER: EBV-encoded RNA; CR2 or CD21: complement receptor type 2; LMP: latent membrane protein; miRNA: microRNA.
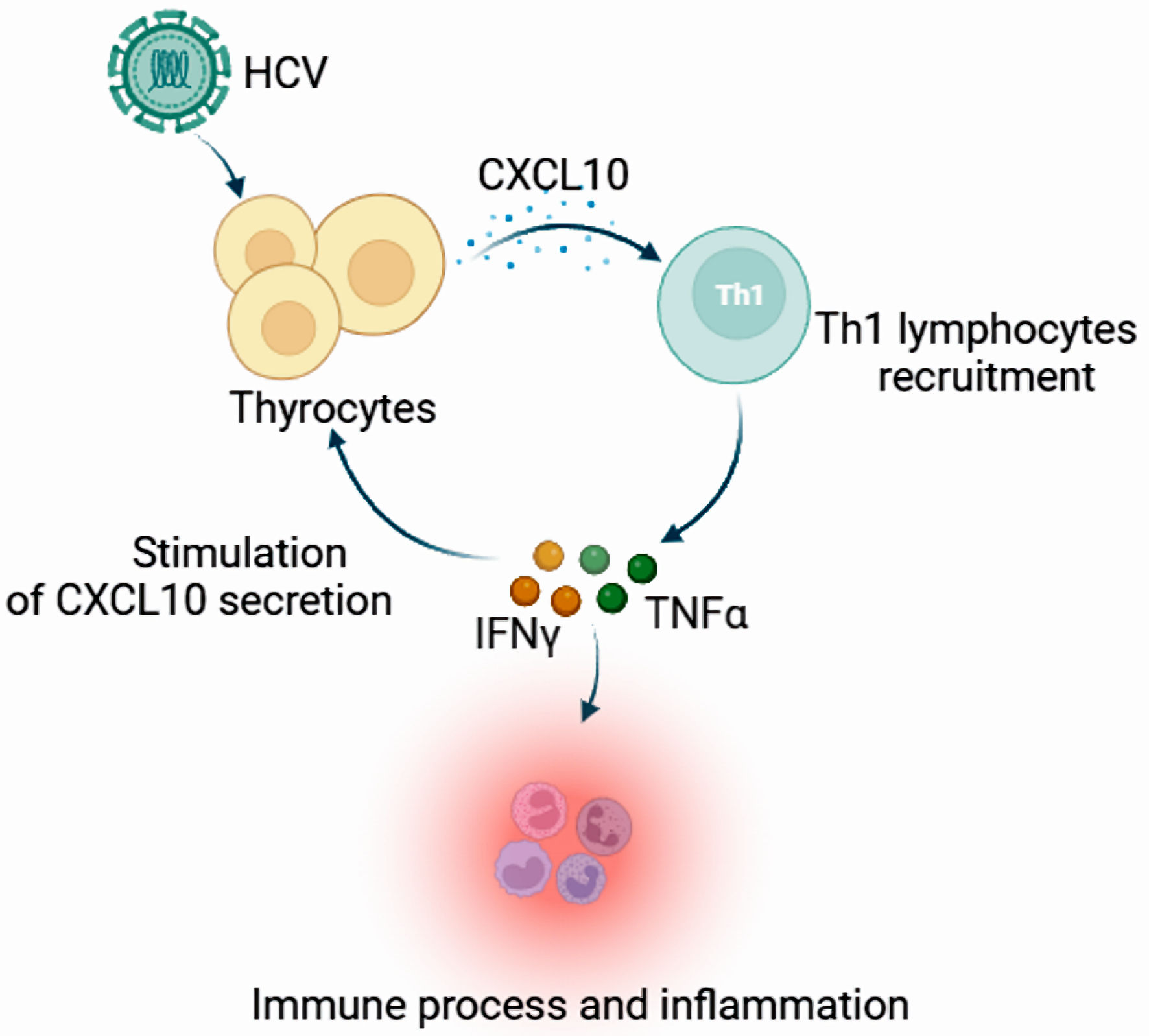
Figure 2. The expression and function of CXCL10 in the appearance of autoimmune thyroid disorders. Chronic HCV infection may upregulate CXCL10 expression and secretion in infected thyrocytes, recruiting Th1 lymphocytes that may be responsible for enhanced IFN-γ and TNF-α production, inducing a further CXCL10 secretion by a variety of cells and creating an amplification feedback loop which initiates and perpetuates the immune cascade, and results in the appearance of autoimmune thyroid disorders in genetically predisposed subjects. CXCL10: C-X-C motif chemotactic factor 10; HCV: hepatitis C virus; IFN-γ: interferon-γ; Th1 cells: T helper 1 cells; TNF-α: tumor necrosis factor-α.
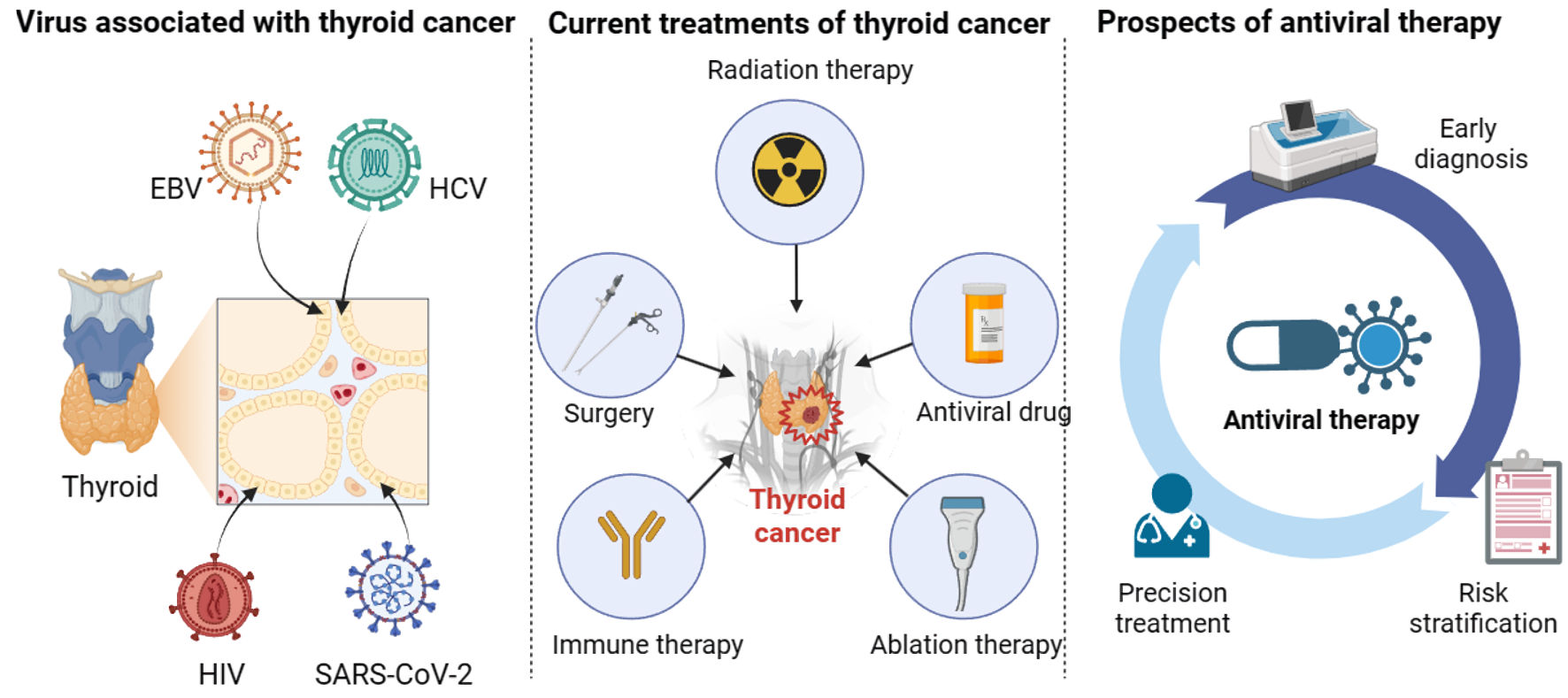
Figure 3. The relationship between viruses and thyroid cancer. Viruses, including EBV, HCV, HIV, and SARS-CoV-2, play an essential role in the progression of thyroid cancer. In addition to surgery, radiation therapy, ablation therapy, and immune therapy, antiviral therapy can facilitate the treatment and management of thyroid cancer patients in terms of early diagnosis, risk stratification, and precision treatment. EBV: Epstein-Barr virus; HCV: hepatitis C virus; HIV: human immunodeficiency virus; SARS-CoV-2: severe acute respiratory syndrome coronavirus 2.