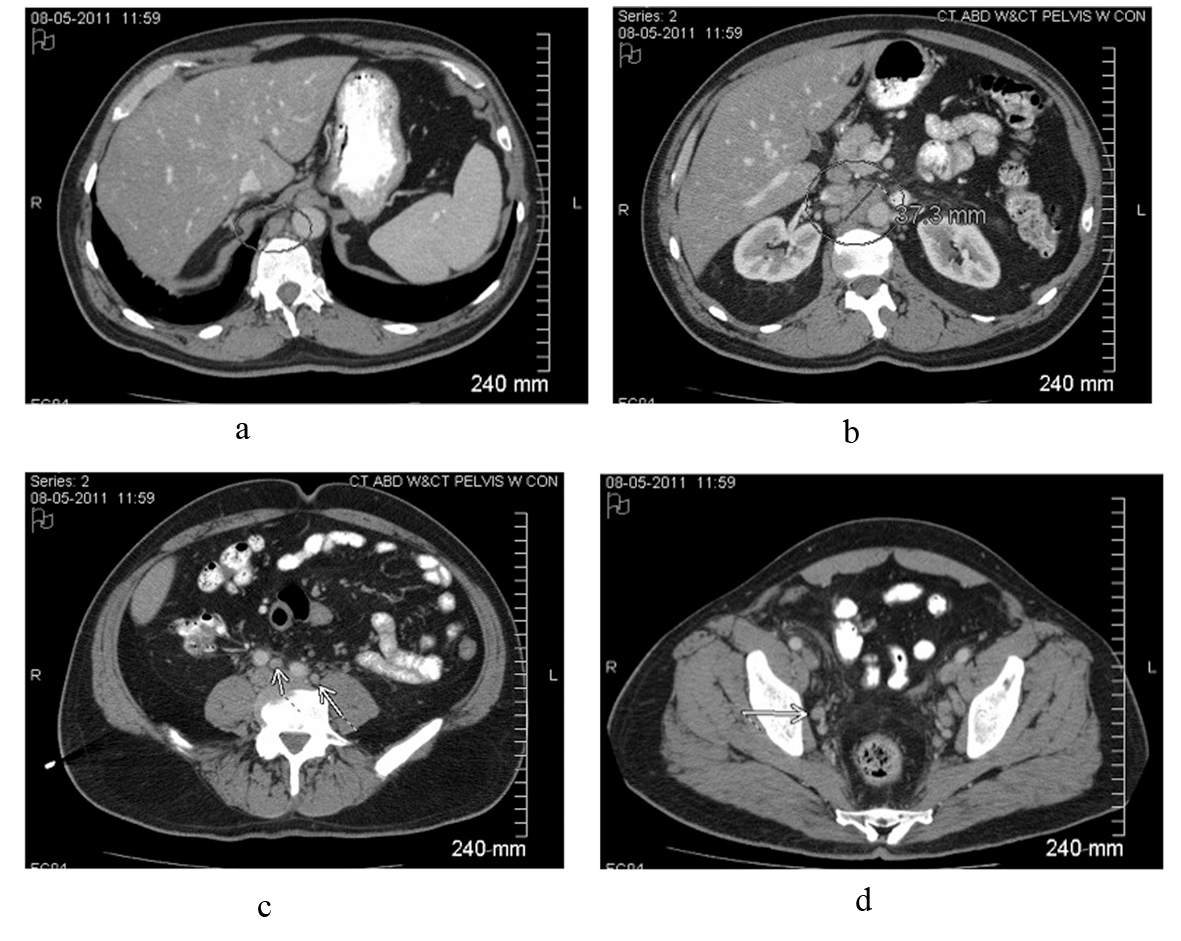
Figure 1. Contrast-enhanced CT scan of the abdomen and pelvis reveals intrabdominal and retroperitoneal adenopathy of uncertain origin. Adenopathy includes right retrocrural, retroperitoneal, celiac, peripancreatic, mesenteric, iliac and pelvic lymph nodes. Upper retroperitoneum reveals confluent nodal mass measuring 37.3 millimeters in image b.
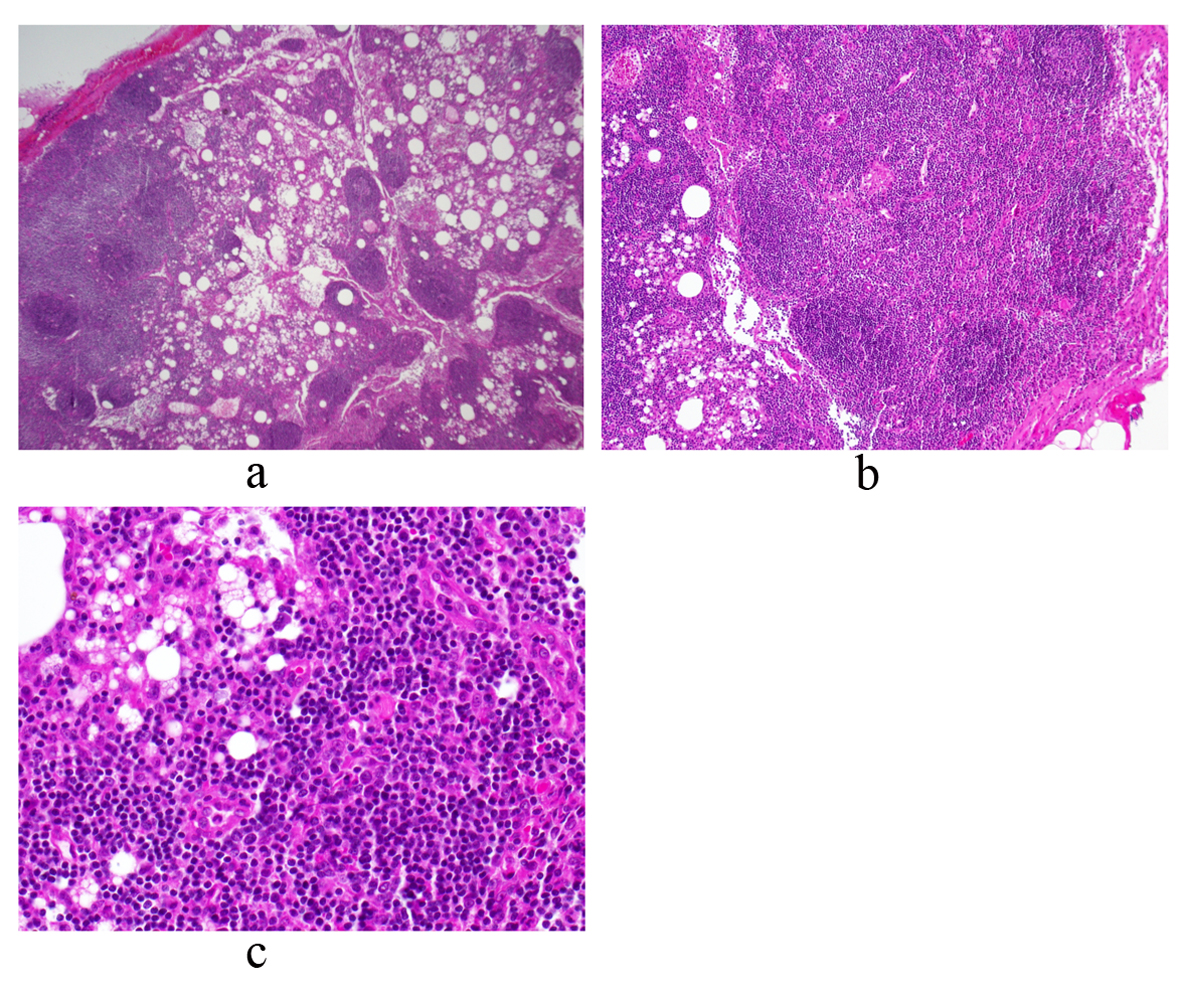
Figure 2. Periaortic lymph node biopsy reveals a mature and polymorphous lymphoid population with some macrophages and normal histologic architecture. There is an intact capsule and no lymphocyte migration outside of the capsule. There are follicles with germinal centers and normal interfollicular cellularity. Photos a, b and c represent low, medium and high power views, respectively.
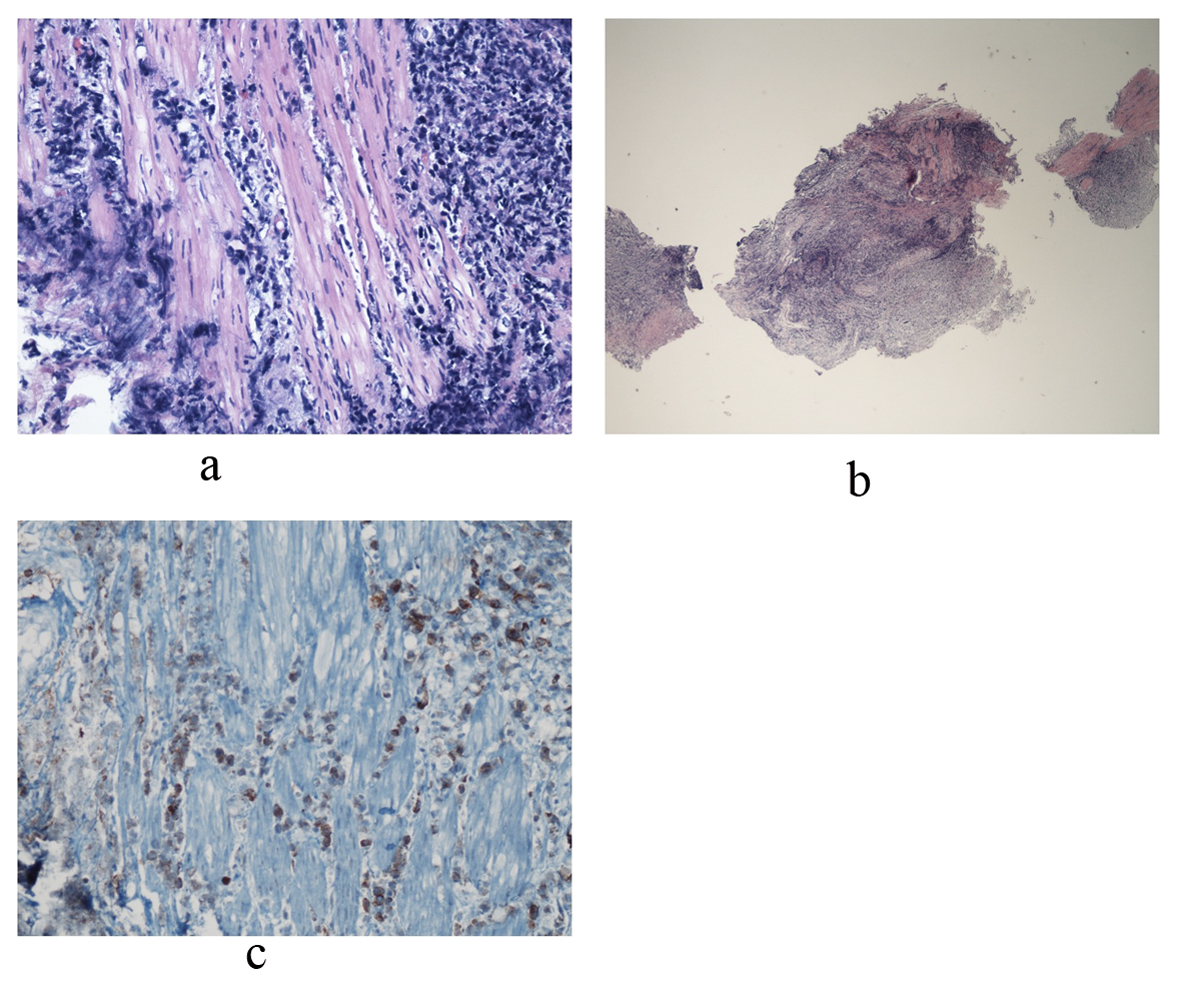
Figure 3. Bladder biopsy sections reveal a dense infiltrate composed of large abnormal lymphoid cells at low and medium power views. Photo a shows diffuse, ragged infiltration of bladder muscle by cells with dark nuclei and moderate size. An example of these cells is represented in photo b. Immunohistochemical stains showed that these large cells are positive for CD45, CD3, CD5, CD4, and CD30. CD30 positive cells are represented in photo c. Occasional large cells are also positive for ALK-1. They are negative for CD20, CD8, CD34, Tdt, CD56, pankeratin, synaptophysin and chromogranin. Findings are consistent with an ALK+ anaplastic large cell lymphoma.