Figures
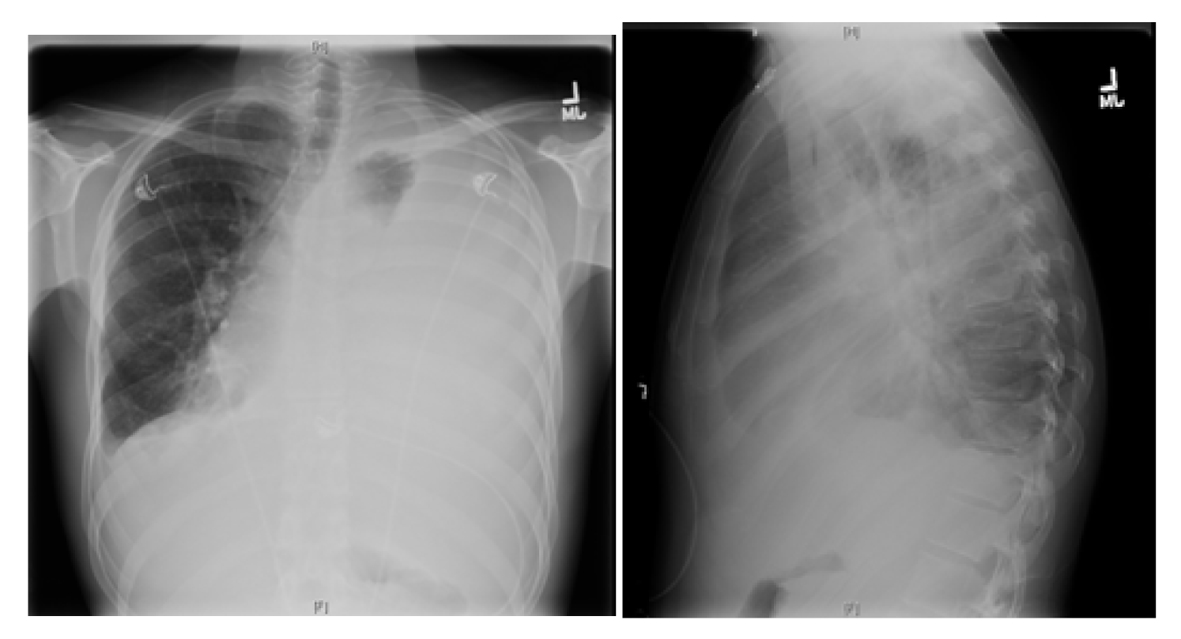
Figure 1. X-ray chest showing near complete opacification of left lung due to massive pleural effusion with shift of mediastinum to right.
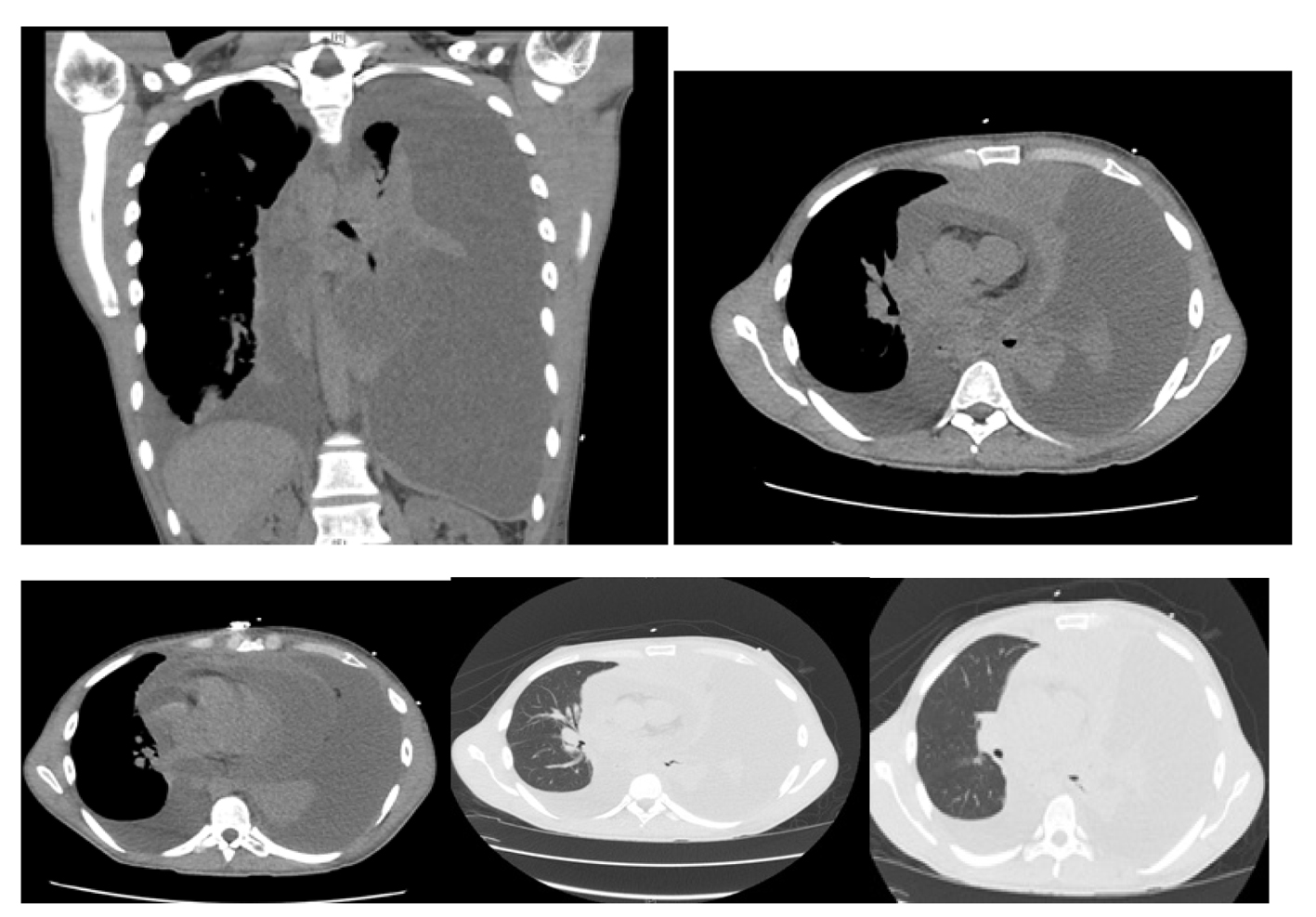
Figure 2. Computer tomography of the chest showing massive left pleural effusion, moderate right pleural effusion, massive pericardial effusion and a mass arising in the anterosuperior mediastinum.
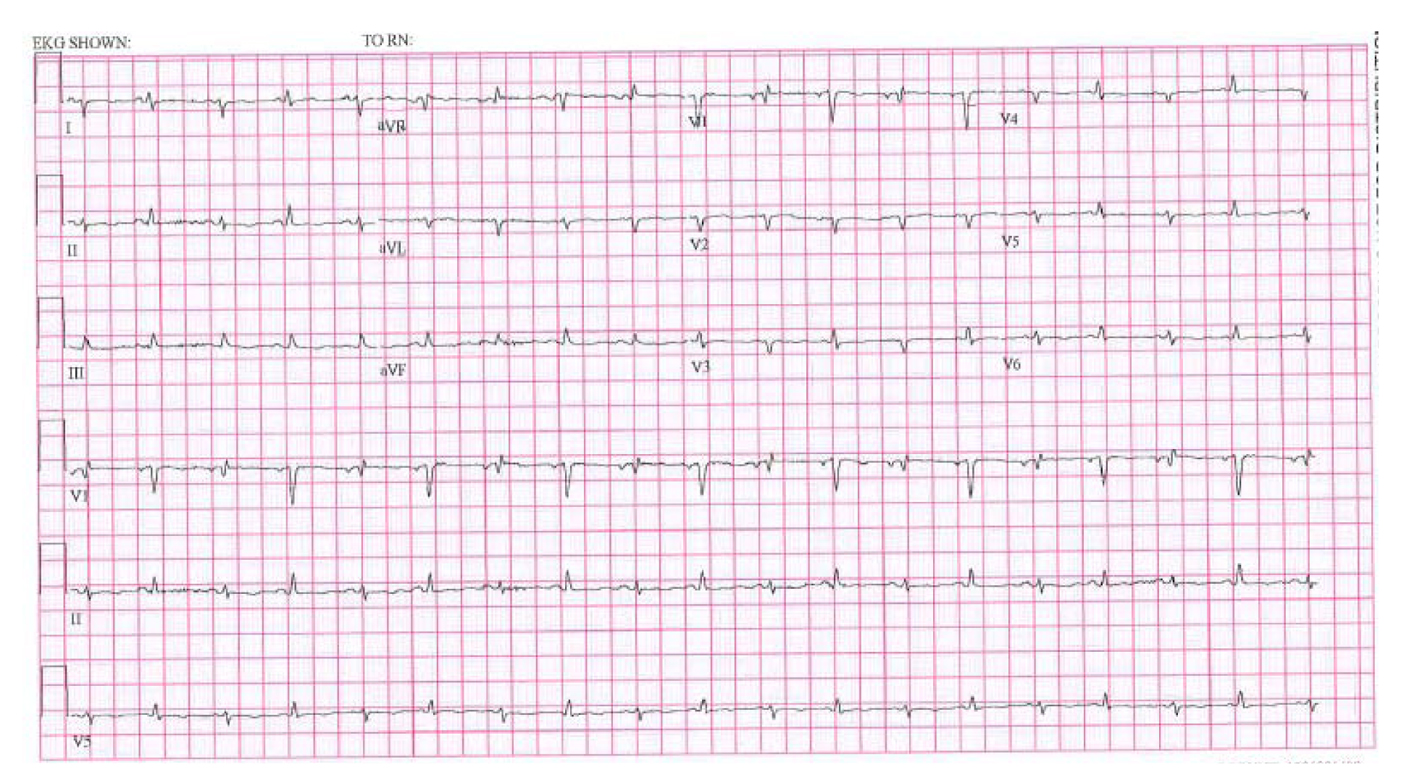
Figure 3. EKG showing low voltage, electrical alternans and sinus tachycardia.
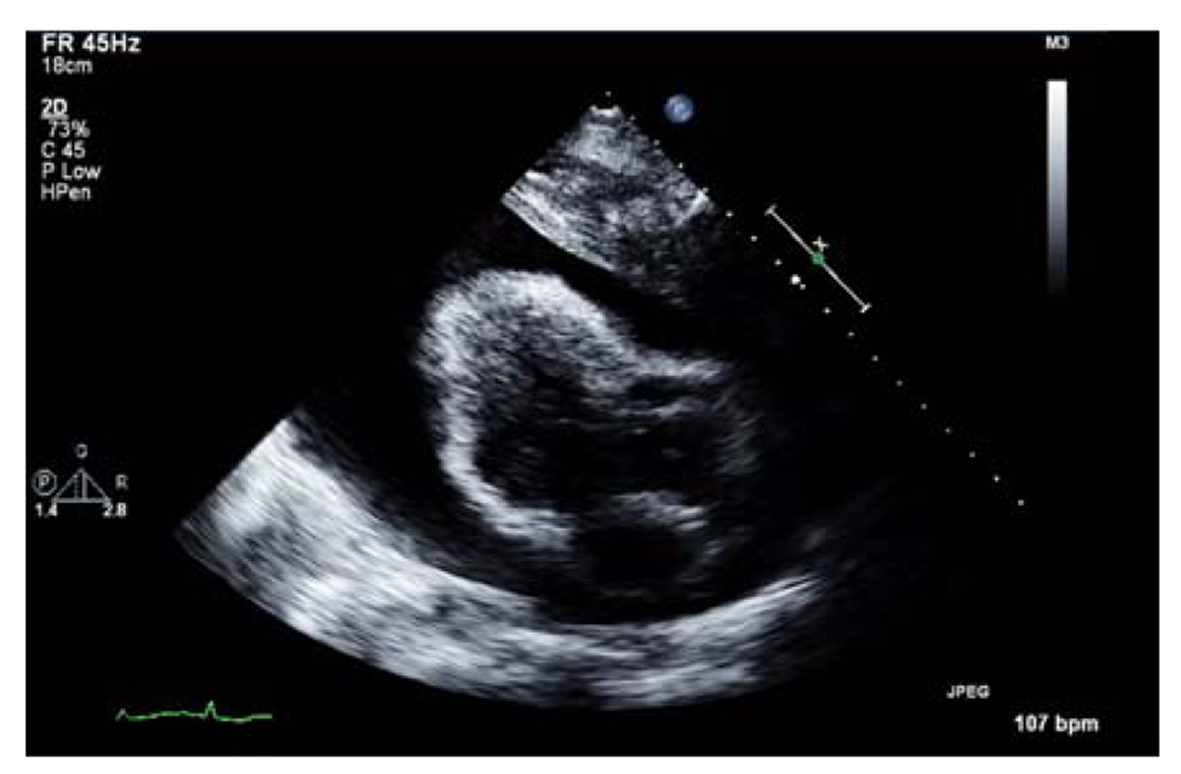
Figure 4. Transthoracic echocardiogram showing massive pericardial effusion.
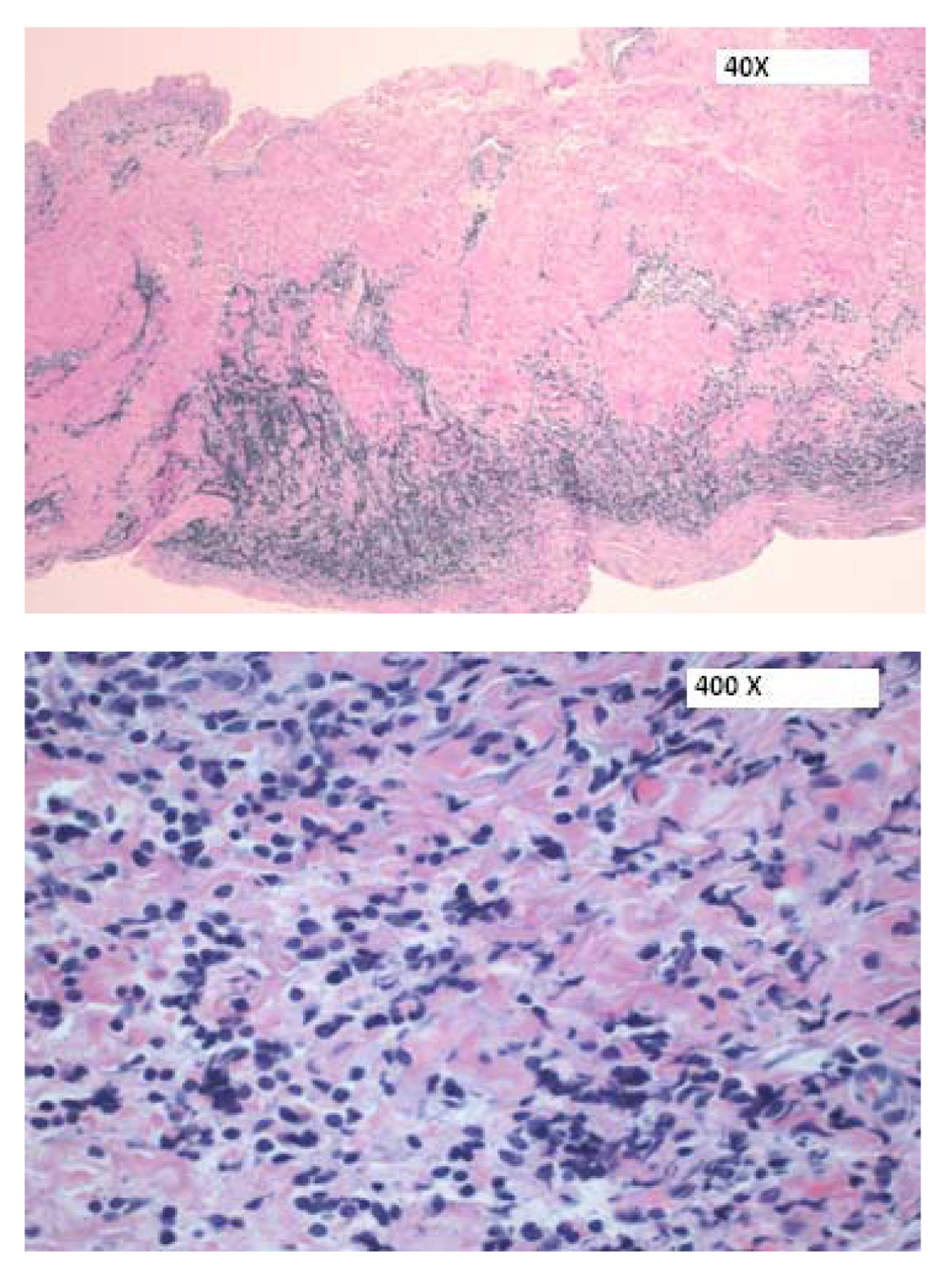
Figure 5. H&E sections of the pericardium showing a focal infiltrate of medium-sized cells within the pericardial wall.
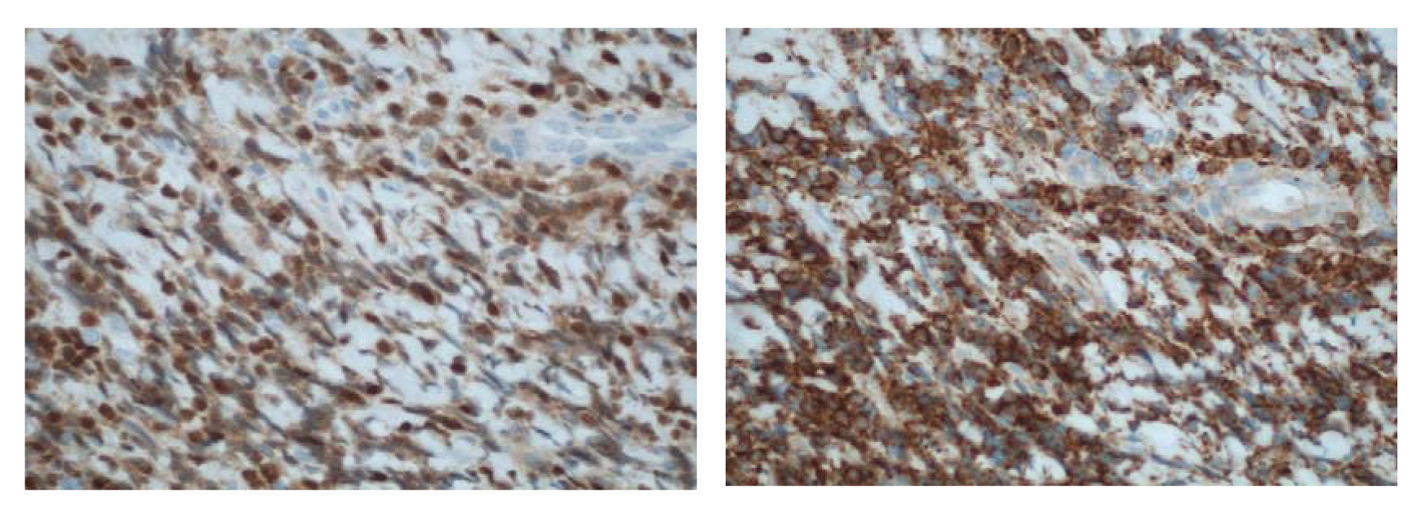
Figure 6. (× 400) Immunohistochemical stains showing (a) an immature CD99+, (b) TdT+ population consistent with a T-cell LBL.
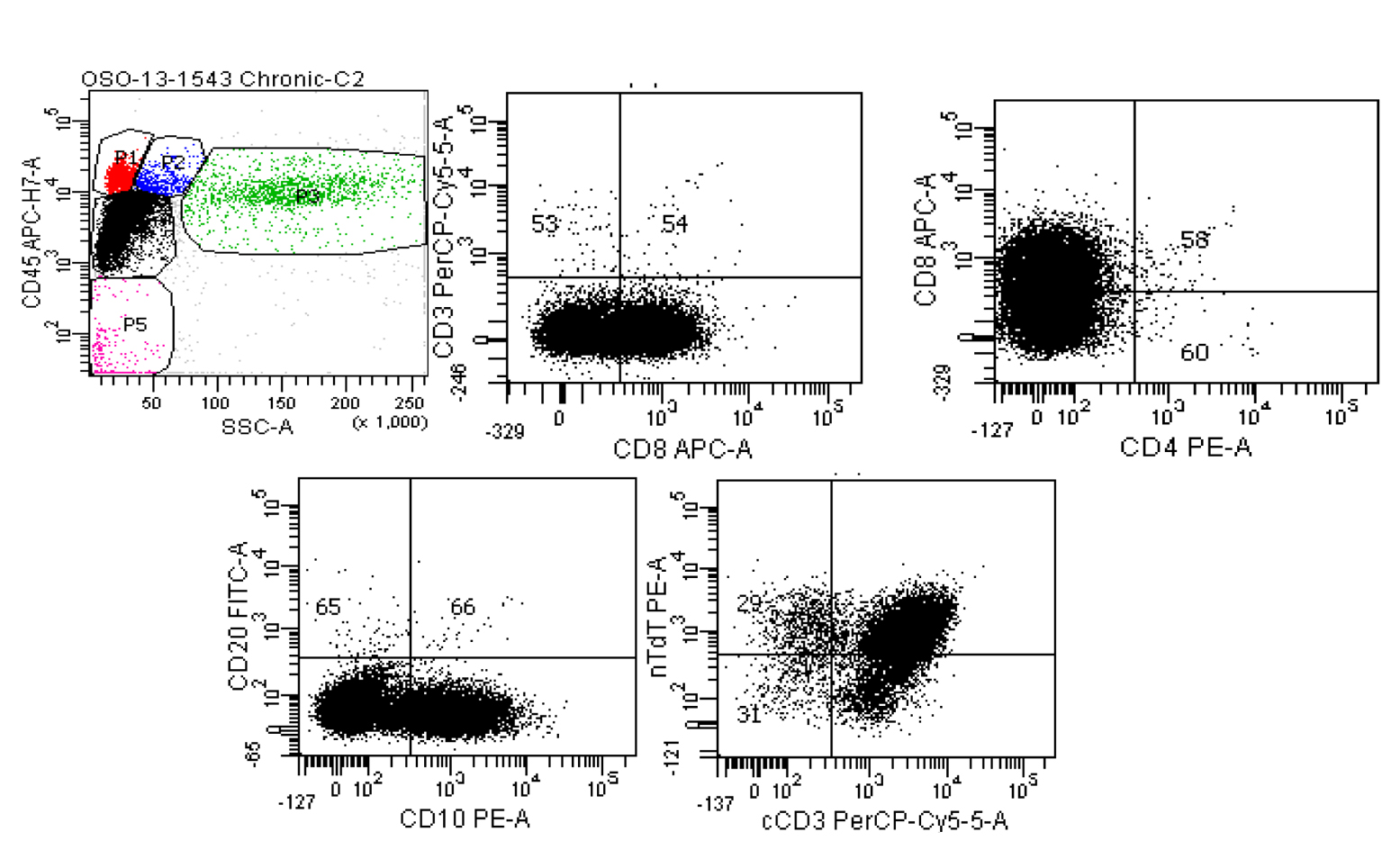
Figure 7. Six color BD FACSCanto II of pericardial fluid. Top left: Ungated CD45 vs. side scatter shows a large population (black dots) in the dim CD45/low side scatter (blast) gate. Top middle: Gating only this dim CD45 population show the cells are negative for surface CD3, positive for CD8, negative for CD4 (top right) and positive for CD10 (lower left). The lower right scattergram shows that although the population of interest was negative for surface CD3, cytoplasmic CD3 is present along with nuclear terminal deoxynucleotidyl transferase (nTdT).
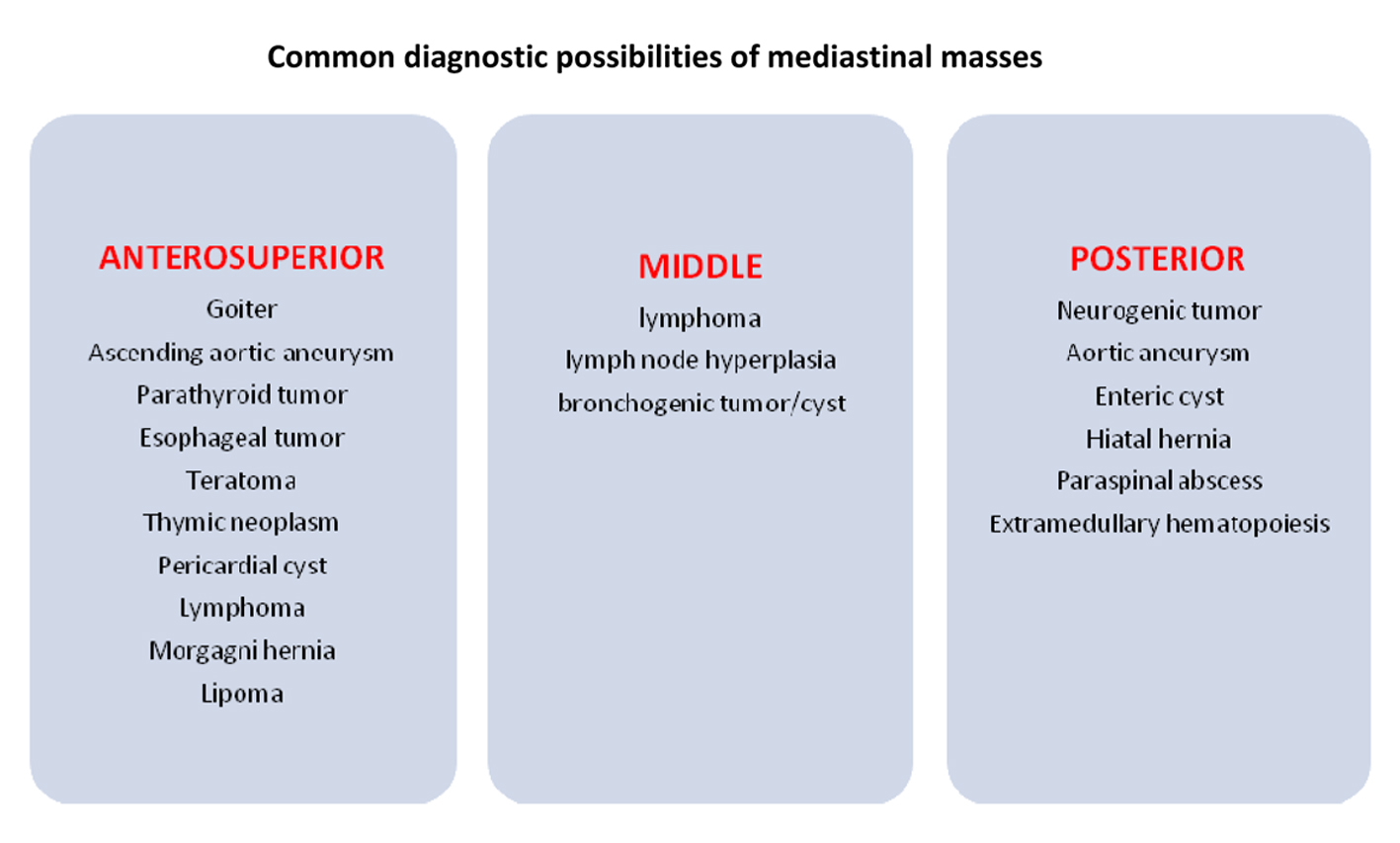
Figure 8. Differential diagnosis for a mediastinal mass.