| Etiology | Acquired urachal remnant disease | Acquired urachal remnant disease |
| Occurrence in symptomatic urachal masses in adults [6] | 35% | 51% |
| Gender predilection | Unknown | Two-thirds in men |
| Age predilection | Unknown | 40 - 70 years |
| Presentation | Dysuria, palpable abdominal mass. | Hematuria, palpable abdominal mass |
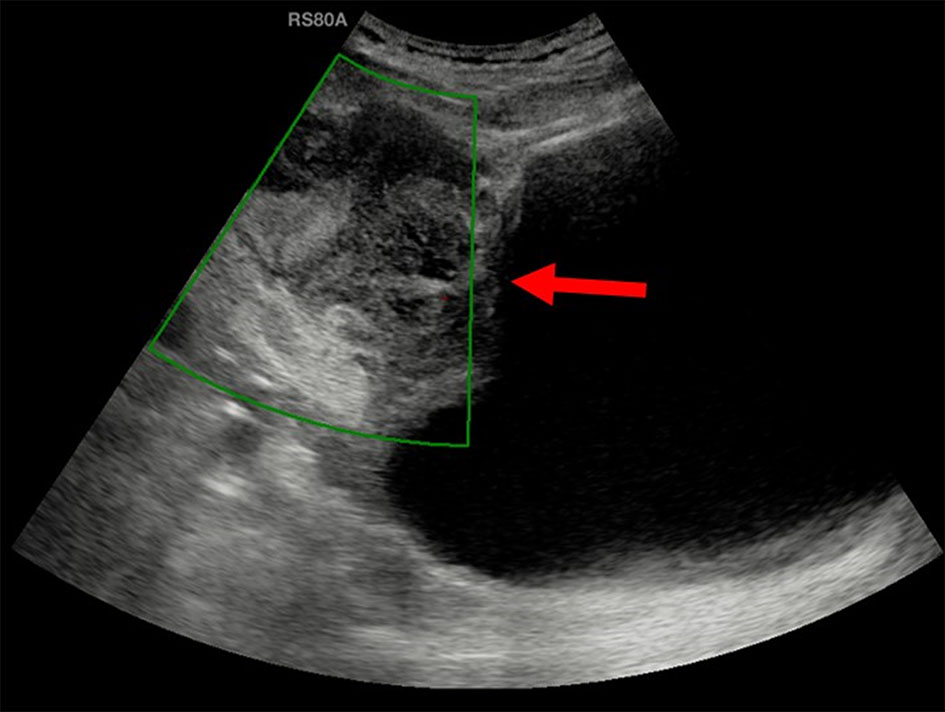
| Ultrasound | Complex heterogeneous echogenic mass in the characteristic location with occasional intralesional gas | Fluid filled cavity in characteristic location with mixed echogenicity and calcifications |
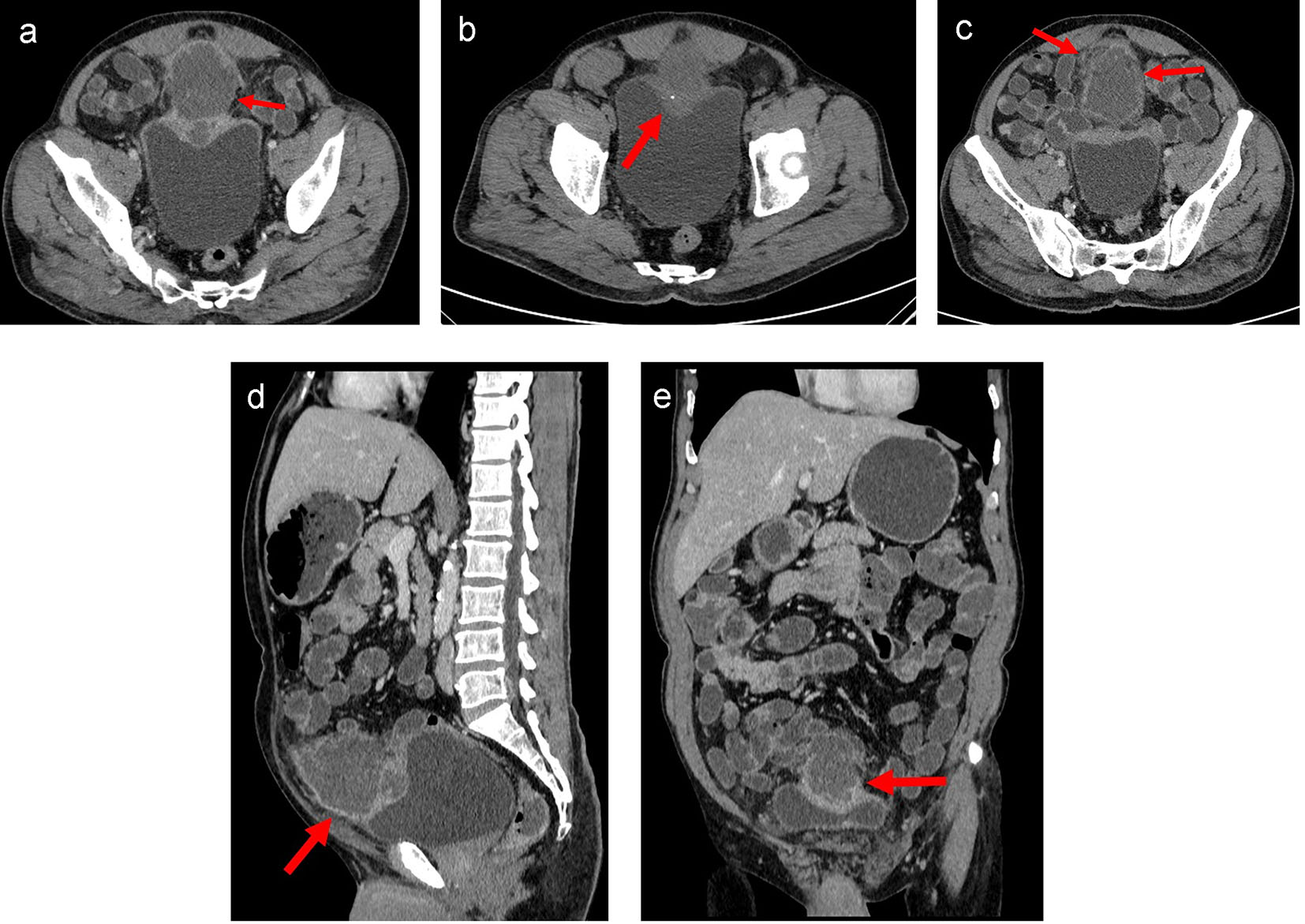
| CT and MRI | Ill-defined heterogeneous enhancing mass with surrounding inflammation | Mixed solid cystic mass with calcifications (70%) and frequent bladder wall invasion |
| Prognosis | Good prognosis. No additional follow-up required. | Good prognosis in early completely resected cases. The 5-year survival rate in locally advanced and distant metastasis is 6.5-15%. |