

| World Journal of Oncology, ISSN 1920-4531 print, 1920-454X online, Open Access |
| Article copyright, the authors; Journal compilation copyright, World J Oncol and Elmer Press Inc |
| Journal website http://www.wjon.org |
Case Report
Volume 7, Number 4, August 2016, pages 91-93
Learning From Mistakes: Importance of a Multidisciplinary Group, A Case Report
Donato Pezzullaa, c, Claudio Scoglioa, Raffaella Capassob, Fabrizio Cioceb, Assunta Sicab, Salvatore Cappabiancab
aSezione di Radioterapia Oncologica, Dipartimento di Medicina Interna Clinica e Sperimentale “Magrassi - Lanzara”, Seconda Universita di Napoli, Via Costantinopoli 104, 80135, Italy
bSezione di Diagnostica per Immagini, Dipartimento di Medicina Interna Clinica e Sperimentale “Magrassi - Lanzara”, Seconda Universita di Napoli, Piazza Miraglia, 2. 80138, Naples, Italy
cCorresponding Author: Donato Pezzulla, Sezione di Radioterapia Oncologica, Dipartimento di Medicina Interna Clinica e Sperimentale “Magrassi - Lanzara”, Seconda Universita di Napoli, Via Costantinopoli 104, 80135, Italy
Manuscript accepted for publication August 10, 2016
Short title: Importance of a Multidisciplinary Group
doi: http://dx.doi.org/10.14740/wjon968e
| Abstract | ▴Top |
There have been significant advances in the diagnosis and treatment of breast cancer over the past 20 years, due to increased knowledge about the biology and molecular changes in breast cancer. These advances have increased the complexity of treatment decision-making for individual women, and reinforced the need for a team approach to treatment decision-making. We report the case of an 80-year-old woman with a recidive invasive ductal breast carcinoma of high grade. In October 2015, she discovered an indolent breast bulk through self-examination and in the December of the same year, after the routine staging exams, she undergone a quadrantectomy and a limphoadenectomy. In March 2016, the patient was sent to our structure for a cycle of radiation therapy by her oncologist, even though a suspected lesion was seen on the thoracic wall on recent computed tomography scans. Our aim was to show an example about the importance of collaboration and multidisciplinary group in treating cancer.
Keywords: Breast cancer; Multidisciplinary group; Secondary lesion
| Introduction | ▴Top |
There have been significant advances in the diagnosis and treatment of breast cancer over the past 20 years, due to increased knowledge about the biology and molecular changes in breast cancer [1].
These advances have increased the complexity of treatment decision-making for individual women, and reinforced the need for a team approach to treatment decision-making.
Multidisciplinary care probably improves patient outcomes by influencing various aspects of care. These factors include adherence to guidelines, increased surgical volume and experience, and improved interdisciplinary working [2].
Barriers to effective teamwork and poor decision-making include excessive caseload, low attendance at meetings, lack of leadership, poor communication, role ambiguity, and failure to consider patients’ holistic needs [3].
| Case Report | ▴Top |
We report the case of an 80-year-old Caucasian woman with a relapsed invasive ductal breast carcinoma of high grade.
In October 2015, she discovered an indolent breast bulk through self-examination and in the December of the same year, after the routine staging exams, she undergone a quadrantectomy with limphoadenectomy. In March 2016, the patient was sent to our structure to plan a cycle of radiation therapy by her oncologist.
In order to adequately plan the radiation therapy, we examined the recent diagnostic examinations performed. Among post-operative studies, we found a computed tomography (CT) scan performed in February 2016, which showed a nodular lesion (10 - 11 mm) of the left thoracic wall, signaled by the radiologist. However, the images were not so clear and the fact that the oncologist, even though aware of the presence of this lesion, suggested the irradiation therapy, putting us in doubt.
In order to obtain a full view of the situation and determinate the correct treatment, surgery or radiotherapy, we decided to present the doubtful case to the radiologists of radiological department of our structure for a second evaluation.
They confirmed that CT images had a low quality and expressed the necessity of a thoracic wall magnetic resonance imaging (MRI).
While organizing the execution of the MRI, we had to explain the situation to a very anxious lady that did not understand why we did not want to treat her, when the oncologist told her that there was nothing to worry.
The exam showed a lesion of 27 × 13 mm at the level of the left great breastplate having heterogeneous contrastographic impregnation of intravenous contrast medium suggesting a secondary nature (Fig. 1). So we guided the patients to a surgeon to remove the lesion and a month after we were informed that the patient undergone a new surgery.
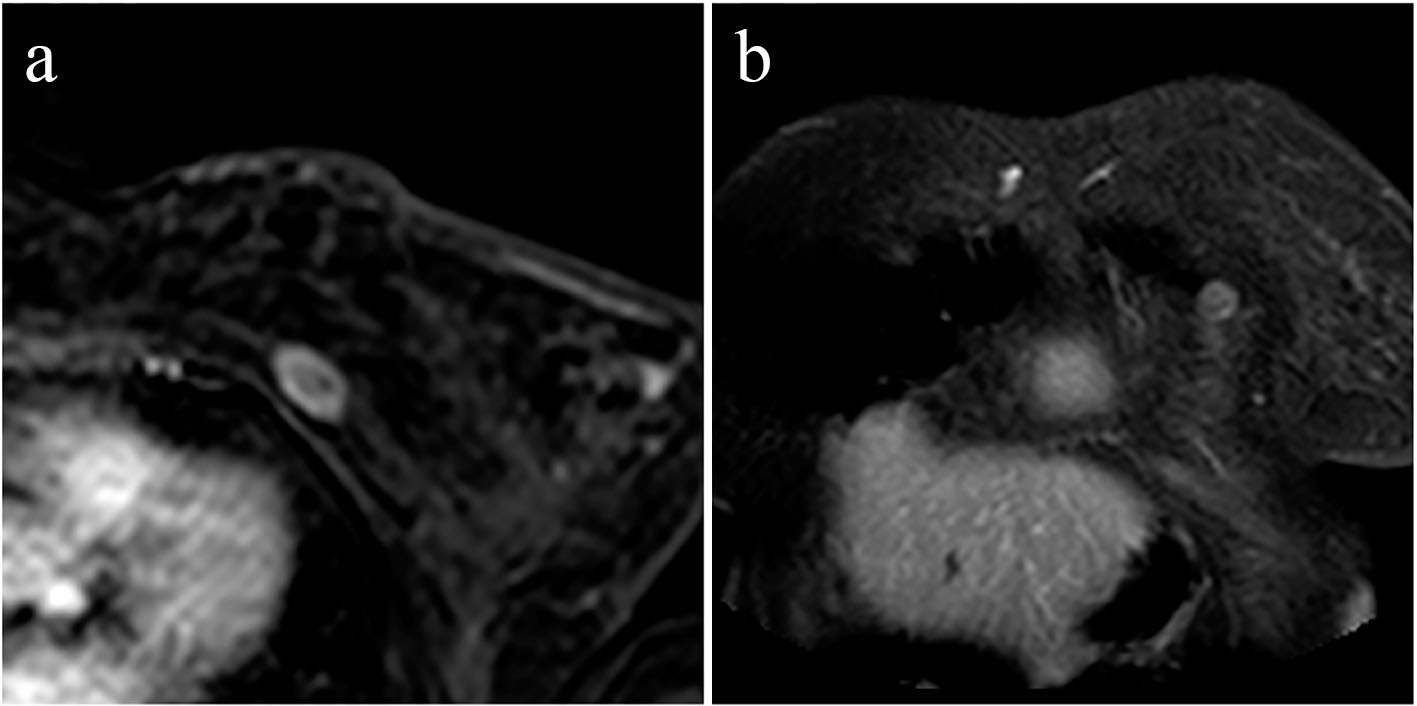 Click for large image | Figure 1. Magnetic resonance imaging of the thoracic wall: post-contrast T1-weighted axial (a) and coronal (b) images showing a nodular enhancing lesion of the left major pectoralis muscle. |
| Discussion | ▴Top |
Previous management of cancer patients before the idea of multidisciplinary team management was conceived involving the referral of patients from one clinician to another at various stages of diagnosis and treatment without an integrated approach, which can be an overwhelming and confusing experience for a patient [4].
A specialist team approach to breast cancer management may lack randomized controlled trial evidence of effectiveness, but is considered superior based upon both clinical consensus and research evidence [3].
As we can see in this case, there has been a lack of teamwork: the surgeon, after removing part of the gland, sent the patient to the oncologist who, even saw an unclear situation in the CT scan, sent her directly to our structure for the radiation therapy. Both the surgeon and the oncologist acted alone without consulting each other or colleagues of other disciplines, despite the suspected CT finding and avoiding to studying in deep the situation.
We do not know if the previous specialists considered the CT founding only an artifact or they undervalued it, but acting this way we could have two differrent results: if the lesion was only a CT artifact then the patient would have had the right condition and all the advantage for the radiation therapy; on the other hand, if the lesion was real, then the woman would have had to undergo a mastectomy.
In the latter case, the patient would suffer a further stress and lose the perfect treatment timing.
Accordingly with the international guidelines, we think that the case should have been analyzed by a team of different fields.
In this situation, in relation to doubtfull CT findings, MRI would have been considered the main choice to resolve the dilemma by a multidisciplinary experienced team. MRI execution soon after CT scan should have allowed to better assess the extent of disease, whether operable and how operable, and guiding surgery [5].
The team would have addressed the patients from the start to an appropriate surgical treatment, followed by hormonal therapy and, in the case of a conservative surgery, a cycle of radiation therapy [6].
Another inportant element that we should consider is the patient’s point of view: in all this story the lady had been sent from a specialist to anonter one, everyone in different structures, losing several months in between their consulences. All this uncertinity caused a very stressfull situation for her and her family.
In our opinion, this story is a perfect example that shows the importance of a multidisciplinary team cooperation: it would have handled the case in a better and safer way for the patients, probably avoiding to this woman to wander from a specialist to another and to undergo surgery twice.
Conflicts of Interest
Authors declare that there are no conflicts of interest regarding the publication of the article.
| References | ▴Top |
- Polyak K. Breast cancer: origins and evolution. J Clin Invest. 2007;117(11):3155-3163.
doi pubmed - Kesson EM, Allardice GM, George WD, Burns HJ, Morrison DS. Effects of multidisciplinary team working on breast cancer survival: retrospective, comparative, interventional cohort study of 13 722 women. BMJ. 2012;344:e2718.
doi pubmed - Taylor C, Shewbridge A, Harris J, Green JS. Benefits of multidisciplinary teamwork in the management of breast cancer. Breast Cancer (Dove Med Press). 2013;5:79-85.
doi - Abdulrahman GO, Jr. The effect of multidisciplinary team care on cancer management. Pan Afr Med J. 2011;9:20.
doi - Saunders C, Taylor D. Expanding the indications for MRI in the diagnosis and treatment of breast cancer: what is best practice? J Med Radiat Sci. 2015;62(1):47-53.
doi pubmed - Ciaglia GF, Martino A, Sayad K, Scoglio C, Pezzulla D, Cappabianca S. Management of Bone Metastases From Breast Cancer in Upper and Lower Body at the Same Time: A Case Report. World J Oncol. 2016;7(2-3):57-58.
doi
This is an open-access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
World Journal of Oncology is published by Elmer Press Inc.