

| World Journal of Oncology, ISSN 1920-4531 print, 1920-454X online, Open Access |
| Article copyright, the authors; Journal compilation copyright, World J Oncol and Elmer Press Inc |
| Journal website https://www.wjon.org |
Review
Volume 13, Number 3, June 2022, pages 103-106

Carcinosarcoma of the Gallbladder: A Rare Tumor
Subhi Mansoura, Elena Derkacha, Valerya Abergilb, Safi Khuria, c, d
aGeneral Surgery Department, Rambam Health Care Campus, Haifa, Israel
bOperating Room, Rambam Health Care Campus, Haifa, Israel
cHPB and Surgical Oncology Unit, Surgery Department, Rambam Health Care Campus, Haifa, Israel
dCorresponding Author: Safi Khuri, HPB and Surgical Oncology Unit, General Surgery Department, Rambam Health Care Campus, Haa’leya Hashniya, Haifa 31096, Israel
Manuscript submitted May 14, 2022, accepted June 13, 2022, published online June 22, 2022
Short title: Carcinosarcoma of the Gallbladder
doi: https://doi.org/10.14740/wjon1495
- Abstract
- Introduction
- Pathological Diagnosis of Gallbladder Carcinosarcoma
- Historical Perspectives
- Methods
- Radiological Findings
- Management and Prognosis
- Summary
- References
| Abstract | ▴Top |
Malignant tumors of the gallbladder are rare, with adenocarcinoma being the most common histological subtype. Carcinosarcoma of the gallbladder, first described in 1907 by Landsteiner, is an extremely rare tumor which comprises less than 1% of the uncommon gallbladder cancers. This unique type of tumor can develop at any major organ, with the uterus being the most common one. Being a tumor that contains epithelial and mesenchymal components, histopathological diagnosis of such rare tumor is a challenging issue. Up to date, there are less than 100 cases of gallbladder carcinoasarocoma reported in the English literature. Therefore, experience and knowledge regarding this rare disease are very limited. Due to the fact that gallbladder carcinosarcoma is a rare and highly forgotten tumor, this article aims to review the English literature to increase awareness of the treating physician to improve diagnosis, management, as well as overall survival.
Keywords: Gallbladder; Carcinosarcoma; Rare tumor; Late diagnosis; Carcinoma; Sarcoma
| Introduction | ▴Top |
Primary carcinosarcoma of the gallbladder is an extremely rare tumor, accounting for less than 1% of primary gallbladder tumors. This rare entity of tumor is very aggressive with an overall survival rate of 2.9 - 6 months, and usually diagnosed late [1]. Gallbladder carcinosarcoma can spread either hematogenously by lymphatic invasion or by direct invasion to adjacent organs and vessels. The precise mechanism for the development of such tumor is still unknown. It is hypothesized that gene expression patterns along with genetic alterations are likely to account for epithelial to mesenchymal transition and sarcomatous changes in already established cholangiocarcinoma [2]. Preoperative diagnosis is very challenging, even with the use of different radiological exams. The precise diagnosis of gallbladder carcinosarcoma is usually made following pathological analysis of the resected specimen. An immunohistochemical stain examination usually shows epithelial (carcinomatous) component positive for cytokeratin and mesenchymal (sarcomatous) component positive for vemintin. Up to date, less than 100 cases of primary gallbladder carcinosarcoma were reported in the English literature.
| Pathological Diagnosis of Gallbladder Carcinosarcoma | ▴Top |
Primary malignant tumors of the gallbladder, the most common biliary tumors, are rare. The most common histological type is adenocarcinoma, comprising about 80-95%, followed by anaplastic (2-7%), squamous cell (1-6%), adenosquamous (1-4%) and small cell (1-3%) subtypes. Primary gallbladder carcinosarcomas are extremely rare tumors, with less than 1% prevalence rate [3, 4]. Carcinosarcoma, known also as pseudosarcoma, spindle cell carcinoma or sarcomatoid carcinoma, is a rare tumor that is characterized by malignant epithelial cell as well as mesenchymal tumor cell components. This rare entity of gallbladder tumor was included sometimes by pathologists in the category of undifferentiated gallbladder carcinoma. Adenocarcinoma is the most common epithelial component, while spindle cell type is the most common mesenchymal component [5]. These tumors most commonly affect the gynecological organs (mostly the uterus) or the otolaryngological organs (e.g., thyroid gland) [6-8]. Other organs that could be affected include the esophagus, kidneys, pancreas, and upper respiratory tract.
| Historical Perspectives | ▴Top |
The first case of gallbladder carcinosarcoma was reported by Karl Landsteiner in 1907 [9]. Since the first report and up to 2010, a paucity of gallbladder carcinosarcoma cases were reported in the English literature. In 2008, Zhang et al [3] was the first to publish a meta-analysis of 68 cases of gallbladder carcinosarcoma. In his study, Zhang et al concluded that race (Japanese vs. non-Japanese) and tumor size are important prognostic factors which could be used for prognosis issues. Since Zhang et al’s publication and up to the date of this article publication, very few articles in the form of case reports or case series discussing gallbladder carcinosarcoma were reported.
| Methods | ▴Top |
Due to the fact that carcinosarcoma of the gallbladder is an extremely rare tumor, the aim of this study is to review the pertinent and available studies in the English literature in order to try and delineate variable findings that can help in early diagnosis of such tumor, to improve management as well as overall survival.
A search in PubMed was conducted, based on the “PICOS” acronym. Headings and text words were used to identify studies (in the form of case reports or case series) published about carcinosarcoma of the gallbladder.
The following search terms were included: “rare gallbladder tumors”, “gallbladder carcinosarcoma”, “gallbladder malignancy”, “carcinosarcoma”, and “rare carcinosarcoma”.
Initial search of the current literature revealed more than 100 cases of gallbladder carcinosarcoma. Following exclusion of non-English articles, non-related topics and excluding non-case reports/case series, only 70 articles including 76 patients were included.
Extracted data included clinical factors (patients’ age, gender, risk factors and clinical presentation), serological tests (liver function tests (LFTs) and tumor markers) and radiological findings by either abdominal ultrasound (US) scan, abdominal computed tomography (CT) scan or abdominal magnetic resonance imaging (MRI) (to determine tumor location within the gallbladder and tumor size).
Clinical presentation
Carcinosarcoma of the gallbladder can develop at any age with a wide age range (40 - 91 years old) and mean age at diagnosis being 66 years old (mainly develops during the sixth decade of life) [10]. It is mainly a disease of females, with female to male ratio of 2.62:1. Most patients present with abdominal pain as a sole chief complaint (41/76 patients, 54%), while the rest (46%) present with a combination of complaints. The most common clinical presentation is right upper abdominal pain (76%), followed by weight loss (29%), nausea and vomiting (25%), fever (17%), obstructive jaundice (10%) and abdominal distention (4%) (Table 1). Two patients (2.6%) presented with the diagnosis as an incidental finding.
 Click to view | Table 1. Demographic Features and Clinical Presentation of Primary Gallbladder Carcinosarcoma |
Biochemical tests
LFTs were reported in most patients (59/76, 77.6%) [10]. Of this subgroup, the majority of patients (31/59, 52.5%) had LFTs within normal limits, while the rest (47.5%) displayed abnormal LFTs. Aspartate aminotransferase (AST) was the most common deranged LFT, elevated in 15 patients (25%), followed by elevated alkaline phosphatase (ALP) in 14 patients (23%), alanine aminotransferase (ALT) in 18% and gamma-glutamyl transferase (GGT) in 10%. Only 10% of patients had high levels of total and direct bilirubin. High levels of serum amylase and lipase were reported as sole abnormal serum levels in one patient each (Fig. 1).
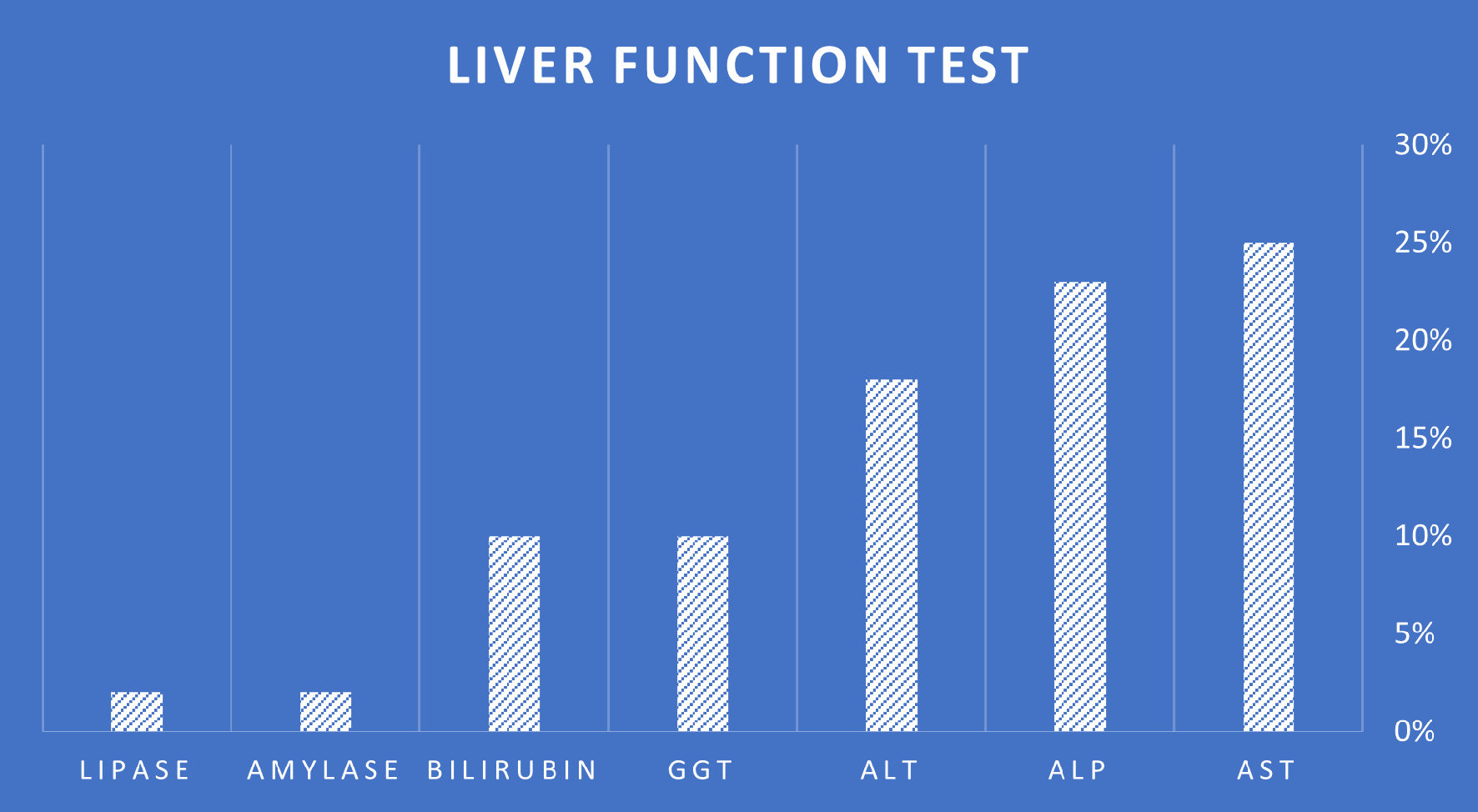 Click for large image | Figure 1. The variables of abnormal liver function tests reported in patients who were diagnosed with primary carcinosarcoma of the gallbladder. AST: aspartate aminotransferase; ALT: alanine aminotransferase; ALP: alkaline phosphatase; GGT: gamma-glutamyl transferase. |
Serum tumor markers, mainly carcinoembryonic antigen (CEA), cancer antigen 19-9 (CA19-9) and alpha fetoprotein (AFP), were available and reported in only 60% of cases. Tumor markers levels were not available in the majority of the early reported cases (prior to the year of 2000). Of the group of patients with available/reported tumor markers (45 patients), the majority (58%) had normal levels of serum tumor markers. CA19-9 was the most common abnormal serum tumor marker, elevated in 12 patients, followed by CEA (five patients), AFP (two patients) and cancer antigen 125 (two patients).
| Radiological Findings | ▴Top |
The presence/absence of gallstones were reported in only 55% of cases (42/76 patients). Of these reports, most patients (83%) had documented gallstones. The size of the tumor on initial diagnosis was reported in 63 patients only, while in 13 cases [11-23] the tumor size was not available. Average tumor size on initial diagnosis by the different radiological tests used (US, CT and MRI scan) has a wide range of variability. In his case report, Gupta et al [24] reported tumor size of 35 × 25 cm on initial diagnosis. On the other hand, tumor size in the case published by Rys et al [25] was 1.5 × 1 cm. The average tumor diameter size for all reported cases is 8.1 cm.
Tumor location within the gallbladder was reported in most cases (47/76 patients), and most commonly diagnosed in the gallbladder fundus (16/47 patients, 34%), followed by the entire gallbladder (30%) and the gallbladder neck in five patients (10%) as the least common.
Initial diagnosis of gallbladder tumor by radiological exams was suspected in most patients (64%), while acute cholecystitis was the initial diagnosis in only 4% of patients.
| Management and Prognosis | ▴Top |
Due to the fact that gallbladder carcinosarcoma is a very rare tumor, up to date, there is no an established consensus regarding the treatment strategy of such tumor. This emphasizes the importance of multidisciplinary approach for this disease. The current treatment of choice is R0 (negative microscopic margins for tumor cells) surgical resection, as no successful treatment has so far been reported with chemotherapy or radiotherapy in terms of overall survival or 5 years survival [26].
Prognosis of gallbladder carcinosarcoma is usually poor, even following aggressive successful R0 surgical resection. Most patients present either with locally advanced or metastatic disease. The most common metastatic sites are the liver and peritoneum [27]. Other reported metastatic sites include the pancreas, adrenal glands, diaphragm and thoracic vertebrae. As mentioned previously, the mean survival following diagnosis is few months. In his review, Okabayashi et al [26] reported 3-year survival rate of 31.1% following curable surgical resection.
| Summary | ▴Top |
Primary carcinosarcoma of the gallbladder is an extremely rare tumor and a forgotten disease for most of the treating physicians. It is a disease of females, in their sixth decade of life, which usually presents with abdominal pain as a sole complaint with normal LTFs and serum tumor markers. Gallstones are common, still, a clear association is yet to be examined.
Although primary carcinosarcoma of the gallbladder is an extremely rare entity, it should be part of the differential diagnosis of primary gallbladder tumors, especially in adult females. Multidisciplinary approach is advised for optimal care of such patients. Authors are encouraged to report such rare cases to gain knowledge of the different characteristics of this disease.
Acknowledgments
None to declare.
Financial Disclosure
None to declare.
Conflict of Interest
The authors have no conflict of interest to declare.
Author Contributions
SM designed the research. VA and ED collected and analyzed the data. SK wrote and approved the final paper.
Data Availability
The authors declare that data supporting the findings of this study are available within the article.
| References | ▴Top |
- Born MW, Ramey WG, Ryan SF, Gordon PE. Carcinosarcoma and carcinoma of the gallbladder. Cancer. 1984;53(10):2171-2177.
doi - Yoo HJ, Yun BR, Kwon JH, Ahn HS, Seol MA, Lee MJ, Yu GR, et al. Genetic and expression alterations in association with the sarcomatous change of cholangiocarcinoma cells. Exp Mol Med. 2009;41(2):102-115.
doi pubmed - Baillie J. Tumors of the gallbladder and bile ducts. J Clin Gastroenterol. 1999;29(1):14-21.
doi pubmed - Khanna M, Khanna A, Manjari M. Carcinosarcoma of the gallbladder: a case report and review of the literature. J Clin Diagn Res. 2013;7(3):560-562.
doi pubmed - Zhang L, Chen Z, Fukuma M, Lee LY, Wu M. Prognostic significance of race and tumor size in carcinosarcoma of gallbladder: a meta-analysis of 68 cases. Int J Clin Exp Pathol. 2008;1(1):75-83.
- Arakawa A, Fujii H, Matsumoto T, Hirai S, Suda K. Loss of heterozygosity in clonal evolution with genetic progression and divergence in spindle cell carcinoma of the gallbladder. Hum Pathol. 2004;35(4):418-423.
doi pubmed - Jonson AL, Bliss RL, Truskinovsky A, Judson P, Argenta P, Carson L, Dusenbery K, et al. Clinical features and outcomes of uterine and ovarian carcinosarcoma. Gynecol Oncol. 2006;100(3):561-564.
doi pubmed - Batsakis JG, Suarez P. Sarcomatoid carcinomas of the upper aerodigestive tracts. Adv Anat Pathol. 2000;7(5):282-293.
doi pubmed - Karl L. Plattenepithelkarzinom und sarkom der gallenblase in einem falle von cholelithiasis. Z Klin Med. 1907;62:427-433.
- Teng TZJ, Chua BQY, Shelat VG. Carcinosarcoma of gallbladder: A world review. World J Clin Oncol. 2021;12(12):1244-1263.
doi pubmed - Kim HH, Hur YH, Jeong EH, Park EK, Koh YS, Kim JC, Kim HJ, et al. Carcinosarcoma of the gallbladder: report of two cases. Surg Today. 2012;42(7):670-675.
doi pubmed - Parreira JM, Siqueira DE, Menacho AM, Pelizzari LL, Santos LC. Carcinosarcoma of the gallbladder: case report. Arq Bras Cir Dig. 2012;25(1):65-66.
doi pubmed - Krishnamurthy V, Shivalingiah SD, Ravishankar S, Manjunath GV. Morphologic heterogeneity in carcinosarcoma of the gallbladder: report of a rare cases. Case Rep Pathol. 2011;2011:929654.
doi pubmed - Kohtani T, Masuda J, Hisaki T, Shimase K, Mizuguchi K. Long-Term Survival of an Elderly Patient with Carcinosarcoma of the Gallbladder after Cholecystectomy. Case Rep Gastroenterol. 2009;3(2):235-239.
doi pubmed - Akatsu T, Ueda M, Shimazu M, Wakabayashi G, Aiura K, Tanabe M, Kawachi S, et al. Primary undifferentiated spindle-cell carcinoma of the gallbladder presenting as a liver tumor. J Gastroenterol. 2005;40(10):993-998.
doi pubmed - Ajiki T, Nakamura T, Fujino Y, Suzuki Y, Takeyama Y, Ku Y, Kuroda Y, et al. Carcinosarcoma of the gallbladder with chondroid differentiation. J Gastroenterol. 2002;37(11):966-971.
doi pubmed - Eriguchi N, Aoyagi S, Hara M, Hashino K, Imamura M, Sato S, Imamura I, et al. A so-called carcinosarcoma of the gallbladder in a patient with multiple anomalies—a case report. Kurume Med J. 1999;46(3-4):175-179.
doi pubmed - Inoshita S, Iwashita A, Enjoji M. Carcinosarcoma of the gallbladder. Report of a case and review of the literature. Acta Pathol Jpn. 1986;36(6):913-920.
doi pubmed - Lopez GE, Strimel W, Herrera-Ornelas L. Carcinosarcoma of the gallbladder: report of a case. J Surg Oncol. 1985;29(4):224-226.
doi pubmed - Yamagiwa H, Yoshimura H, Tomiyama H, Kawahara S, Ito F. [So-called carcinosarcoma]. Rinsho Byori. 1982;30(10):1096-1102.
- Mansori KS, Cho SY. Malignant mixed tumor of the gallbladder. Am J Clin Pathol. 1980;73(5):709-711.
doi pubmed - Higgs WR, Mocega EE, Jordan PH, Jr. Malignant mixed tumor of the gallbladder. Cancer. 1973;32(2):471-475.
doi - Appelman HD, Coopersmith N. Pleomorphic spindle-cell carcinoma of the gallbladder. Relation to sarcoma of the gallbladder. Cancer. 1970;25(3):535-541.
doi - Gupta S, Kori C, Kumar V. Primary carcinosarcoma of the gall bladder: a rare entity. Indian J Surg Oncol. 2016;7(1):101-105.
doi pubmed - Rys J, Kruczak A, Iliszko M, Babinska M, Wasilewska A, Limon J, Niezabitowski A. Sarcomatoid carcinoma (carcinosarcoma) of the gallbladder. Gen Diagn Pathol. 1998;143(5-6):321-325.
- Okabayashi T, Sun ZL, Montgomey RA, Hanazaki K. Surgical outcome of carcinosarcoma of the gall bladder: a review. World J Gastroenterol. 2009;15(39):4877-4882.
doi pubmed - Gao S, Huang L, Dai S, Chen D, Dai R, Shan Y. Carcinosarcoma of the gallbladder: a case report and review of the literature. Int J Clin Exp Pathol. 2015;8(6):7464-7469.
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
World Journal of Oncology is published by Elmer Press Inc.